ABSTRACT
ABSTRACT
| Globally, millions of children suffer from vaccine-preventable diseases. The significant majority of them are from developing countries; nearly one million children miss their childhood vaccines only in Ethiopia every year. A cross-sectional mixed study was conducted in the north Shoa zone of Amhara regional state in Ethiopia to assess factors affecting childhood vaccination coverage.
A total of 371 caregivers were included, and 80.3% of them were female. Twenty caregivers were purposively selected for an in-depth interview. The quantitative data were analyzed using descriptive statistics and logistic regression, and the result was interpreted based on OR, AOR, and p-value at 95% CI. About 218(59%) children were found fully vaccinated. Childhood vaccination status was found to be affected by caregiver knowledge and awareness, such as an awareness of where to get the vaccines AOR 0.33[0.12, 0.9] with a p-value of 0.003, and knowledge of when to start vaccination AOR 0.23[0.11, 0.47] with a p-value <0.001 at 95% CI, being aware of the vaccination schedule; those who can easily recall the next schedule was 7.46 times highly likely to fully vaccinate their children, [3.04, 18.35] with p-value <0.001. The sociodemographic variables were also found to have a significant association with full vaccination status; distance from the health facility between one to four kilometers AOR 0.2[0.07, 0.58] with a p-value of 0.003 and from four to eight kilometers AOR 0.24[0.08, 0.71] with p-value 0.01. Caregivers’ pre and post-health facility visit experience also had a significant association with full childhood vaccination status; hearing peers complain about vaccination service AOR 0.33[0.16, 0.69] with a p-value of 0.003 and those who didn’t receive advice from a health professional on the next vaccination schedule, AOR 0.35[0.12, 0.99] with p-value <0.001. Vaccine promotion had a significant association with childhood vaccination status; caregivers who strongly disagree on the adequacy of vaccine promotion AOR 0.21[0.05, 0.86] with a p-value of 0.029. The qualitative study findings also complement the result of the quantitative study. Moreover, the finding from the qualitative and quantitative study agrees with the desk review result; the gap analysis in the Ethiopian Health Sector Development plan and Immunization Strategy reviews as well as the weakness of the Ethiopian Health Extension Program. To solve the gap identified, the study recommends that the North Shoa Zone and Amhara regional health bureau work with its partners to increase the knowledge and awareness of caregivers and improve access to vaccines and service delivery strategies. 1. IntroductionVaccines are the most important public health discovery in human development. The term vaccine derived from the Latin Variolae (cowpox), which Edward Jenner demonstrated in the second half of the 1700s, could prevent smallpox in humans.(1) Currently, the term vaccine refers to all kinds of biological preparations which can be prepared from living organisms that can enhance immunity to prevent disease or, in some cases, treat disease. Vaccines can be produced and available for use in different forms. Besides the bulk antigen that makes us a certain vaccine, there are several ingredients that will be added, like water. The quality and potency of the vaccine also depend on the additives in the vaccine and other environmental factors. As much as possible, vaccines are formulated so as to be both safe and immunogenic when injected into humans. Vaccines are usually formulated as liquids but may be freeze-dried (lyophilized) for reconstitution immediately prior to the time of injection.(1) 1.1 Background and ContextDespite the discovery of more important technologies in vaccine and management; still, there are gaps that hinder vaccine delivery and achieving the complex immunization schedule where children will receive an entire course of vaccine required to be completed before the age of three years, and in most cases, in less than two years of age.(2) The presence of an effective immunization program in a country can help a country in saving the loss of economy for health care through early prevention of vaccine-preventable diseases. An analysis conducted in China on the measles vaccination campaign in the eastern province of Zhejiang, which provides one dose of measles-rubella vaccine at eight months of age and one dose of MMR at 18 months, estimated that for every dollar spent on immunization, the health system saved about $6.06 in treatment costing, including the cost of treatment complication and longer effect. (3) In the United States alone, nearly 103 million childhood diseases have been prevented due to childhood vaccination programs since 1924. In the US, an investment of one dollar helped to save three dollars from the payer perspective and 10 dollars from the societal perspective.(4) The economic benefits of the vaccine for developing countries are significantly higher than those in developed countries; a recent study conducted on the economic benefits of the vaccine in developing countries indicated that an investment of one dollar on vaccines in developing and middle-income countries would have an economic return of $44.(5) 1.2 Immunization in EthiopiaRoutine immunization started in Ethiopia back in 1980 with six vaccine-preventable diseases, namely measles, diphtheria, pertussis, tetanus, polio, and tuberculosis. The initial target was to increase by 10% annually and reach 100% coverage by 1990; however, this target is still not yet achieved. Full immunization coverage varies from region to region across the country, where the highest coverage is in the Tigray region with 80%, while the lowest is in Somali and Afar regions with less than 5%.(6) After many years of attempts, immunization coverage stood at 71%, according to the World Health Organization and UNICEF estimates in 2018.(7) However, the full immunization coverage of children under the age of two is still not yet able to cross 50%. The immunization coverage in Amhara regional state, the region where this study will be conducted, is one of the lowest as compared to some other regions like Tigray and Addis Ababa. According to the EDHS 2016, the full immunization coverage of the region was 41.6% which is very far behind the World Health Organization recommendation; 90% of children should be fully vaccinated.(8) 1.3 Ethiopian National Health PolicyEthiopian health policy came into shape during the Degree regime that was mainly given priority to disease prevention and control through health promotion and basic curative services with a special emphasis on the rural community. This initiative was started through technical support from the World Health Organization. The initiative, however, was interrupted before it came to full implementation due to regime change, which was replaced by the current regime. The current regime revised the existing health policy to address ten thematic areas emphasising decentralization of services, improving preventive aspect of health care, equitablity, intersectoral colloaboration, etc. The revised health policy has indicated eight areas of focus and special emphasis on family health service, particularly on the health of women and children. One of the sub-area of concern indicated in the national health policy was expanding and strengthening immunization services, and optimizing access and utilization.[1] Despite a significant change in the overall structure of the health system, it seems the health policy is not yet attended to its goal of improving the maternal and child health sector, especially in terms of optimizing access and utilization as the full childhood vaccination coverage remains at its lowest point compared with the World Health Organization recommendation. It is important to evaluate its implementation from a different perspective, and as this study will evaluate the factors that contributed to the low coverage of full childhood vaccination, the finding will be used as an input to revise the policy on optimizing access and utilization of childhood immunization services. 1.4 The Ethiopian National Expanded Program on Immunization (EPI)The Ethiopian EPI is mainly supported by the World Health Organization (WHO), UNICEF, and other partners like Global Alliance for Vaccine and Immunization (GAVI), both technically and financially. Other partners supporting the government of Ethiopia mainly come through these organizations to supply vaccines and cold chain management. The Ethiopian government has mobilized funds to cover the cost of BCG, TT, and 50% of OPV since 2009.(10) Immunization services are being provided in all health facilities, including both government and private hospitals. In public health facilities, routine immunization services are free of charge. In areas where the residents are outside 5 kilometers of the static health facilities, the immunization program is organized in the form of an outreach service. The Reaching Every District (REC) approach was piloted in 2003, and the finding showed there was a significant improvement on the DPT3 planned to scale up in another woreda where there are coverage gaps. This approach was mainly in use in areas where the immunization coverage was too low, like in the Afar, Gambella, and Somali regions of Ethiopia.(10) The existing immunization program document indicated that an advocacy workshop was conducted targeting regions like Gambella, Benishangul, Afar, and Somali regions to address the existing gaps and improve implementation. Despite the presence of leadership to implement immunization programs, financial problems and human resource gaps remain a big challenge in those regions. (10) 1) Problem statement and purpose2.1 Problem statementNearly three million children are dying from the vaccine-preventable disease each year, and the majority of this figure comes from developing countries due to lack of access to the vaccines. Whereas, people in the developed countries are showing complacency to vaccination programs which have impacted disease elimination efforts; for example, measles elimination in developed countries is affected by caregivers’ perception that as the “disease is no longer available in a developed country, a vaccine is not required.” This has caused a disease outbreak in the US recently; the case of a measles outbreak is an example.[2] A significant number of children are not getting a vaccine at all due to several factors like geographic inaccessibility, conflict, and other sociodemographic factors. Among those who started the vaccine, still, another significant proportion of children are missing the consecutive doses. In 2020, about 23 million children were missing their basic vaccination program globally; the data shows an overall increase in the total number of children who missed their vaccination program compared to the report in 2019.(12) The WHO report indicated that about 3.5 million children are missing their first dose of the DPT vaccine, and nearly 3 million children are missing measles first doses in the year 2020 compared to the year 2019 the same year.(13) More than 13 million under-five children live in Ethiopia; nearly one million children are missing life-saving vaccination each year.(14)(15) Studies show that almost 50% of children miss their childhood vaccination, and this varies from region to region and urban to rural.(16) Studies conducted previously showed that the coverage was even worse than the current one, in which as low as only 33% of children got fully vaccinated with high inequitable access to the vaccine. The vaccination coverage in Addis Ababa was seven times higher than in the Afar region.[3] The Ethiopian Health and Demographics Survey (EDHS) 2018 showed that the full immunization coverage of the country stood at 38.5%, while the Amhara region’s full vaccination coverage was 45.8%.(8) A quantitative study conducted in the North Shoa zone to assess factors affecting low measles vaccination coverage showed that the coverage remains at 71%, which is still far behind the World Health Organization recommendation.(18) This study was conducted in a limited area that cannot represent the other district situation, and also, its scope was limited to measles vaccination coverage which will be difficult to generalize for the general population when we talk about childhood vaccination. Generally, while vaccine remains the top solution for reducing child mortality globally, coverage of full childhood vaccination remains unsuccessful. The greatest challenge is found in developing countries, including Ethiopia. The area where this study will be conducted is one of the marginalized areas where road infrastructure and access to health facilities remain poor. In addition, the area is known for different cultural and traditional believe that affect childhood vaccination. 2.2 Justification of the studyConducting this study in the North Shoa Zone of Amhara regional state, particularly in Menz woreda in Ethiopia, will help to explore factors affecting optimum childhood vaccine uptake. The caregivers’ journey to immunization framework preferred to be used during this study to deeply understand what are the barriers at different stages for a caregiver to access full childhood vaccination for their children. Previous studies conducted in Ethiopia either lacked methodology or completeness; most of the studies were conducted to cover the quantitative aspect, while the qualitative remain very important to explain the quantitative findings and adequately support our inquiry. To the best of my knowledge, until this research proposal was developed, there was no study conducted to assess factors contributing to childhood vaccination coverage in the particular area where this study was conducted. Thus, this study will help to determine factors influencing optimum childhood vaccination. Besides, this study will be taken as a reference to study contributing factors for below optimal coverage of childhood vaccination in the future in the same area. 2.3 Purpose of studyThe optimal full vaccination coverage can be affected by several factors, including policies, environmental, societal, and family-level factors. On top of all factors, family-level factors, especially the role of caregivers, particularly mothers in the Ethiopian context, play a significant role. Hence, the purpose of this study focuses on assessing factors affecting the care givers’/mothers’ journey to vaccination, starting from deciding to vaccinate a child to completing full doses of a childhood vaccine. Hence this study assessed caregivers’ sociodemographic factors, knowledge and awareness, decision making and process of vaccination challenges, pre and post-health facility visit experiences, as well as the extent of vaccine promotion. The study was intended to assess these factors both quantitatively and qualitatively from the caregivers’ perspective. Moreover, the purpose of this study was to review the existing policies, immunization strategies, and other relevant guidelines and documents, including the Health Extension Program to link the finding from this research and show gaps with an appropriate recommendation to policy makers. 2.4 Scope of the studyThis study is a cross-sectional conducted from January 15 to February 15 to assess caregivers’ journey to vaccination using qualitative and quantitative methods in selected woredas of the North Shoa Zone. The initial sample size for this study was calculated to be 364, and it was adjusted to 400, considering a 10% nonresponse rate. The data was collected considering four different settings; urban, semi-urban, rural, and remote areas proportionally from selected woredas in the north Shoa Zone. Quantitative data was collected through a house-to-house interview using a semi-structured questionnaire, while the qualitative data was collected through an in-depth interview of 20 purposively selected caregivers among quantitative study participants. Besides the qualitative and quantitative study conducted through primary data collection, the country’s national health policy, national Health Sector Development Plans (HSDPI-IV), National Expanded Program for Immunization(NEPI), and National Health Extension Program (NHEP) were reviewed to link the gaps seen from the study related to the policy and strategies and provide appropriate recommendations. 2) Objective of the study3.1 Primary objectiveThe primary objective of this study was to assess factors influencing childhood vaccination coverage in the North Shoa Zone of the Amhara region in Ethiopia from the perspective of caregivers. This study used the caregiver’s journey to immunization framework developed by UNICEF and its partners to analyze individual, family, and health facility-related factors that can influence the decision of caregivers to fully vaccinate their children. The study was found to be the only research done in this particular area to assess what factors contribute to low coverage of childhood vaccination though the problem has existed for a long time. Hence, this study can be used as a reference for upcoming research in the field. 3.1.1 Specific objective
3.2 Secondary objectiveThe secondary objective of this study is to review country documents related to immunization and provide recommendations for improvement based on the study findings to improve the policy and strategies in the future targeting childhood vaccination. 3) Statement of hypothesis and research questions4.1 Statement of hypothesisThe overall childhood vaccination coverage in Ethiopia is one of the lowest, and full childhood vaccination coverage is the worst, which remains less than 50% nationally. Considering this fact, the researcher believes that the factors contributing for unable to attain full childhood vaccination or optimum childhood vaccination coverage need to be well studied especially in the area where this study will be conducted. The researcher believes that the absence of a previous study in the area has created a gap in policy development and implementation of immunization programs. The researcher believes that a combination of qualitative and quantitative methods will help to explore adequate information on why attaining optimum childhood vaccination coverage remain challenging. Besides, the researcher believes that reviewing the existing national health policy and providing feedback will help fill the gap and revise the existing policy to improve the implementation of the childhood vaccination program. 4.2 Research questionsThe research question address one main question, which deals with the factors contributing to low childhood vaccination coverage, and the second question shows how low childhood vaccination coverage can affect policy development and implementation. Question: How the caregivers’ journey to immunization will be affected by different factors in vaccinating their children during childhood? Furthermore, how the national health policy development and implementation be affected by low full childhood vaccination coverage? To address these two questions, the researcher will study:
5) Literature reviewIn this literature review, keywords were used to search studies and reports documented, including vaccine, vaccination, full vaccination, optimum vaccination, knowledge, attitude, hesitancy, refusal, cost, reminder, and caregiver. Similarly, the following key phrases were also used to search: subjective norm, caregiver experience, perceived behavioral control etc. all literature, including those terms, was searched and considered for review except for studies done before 2000. Evidence about adult vaccines and animal vaccines were excluded from the beginning and not considered for review. 5.1 Sociodemographic factors and optimum childhood vaccine uptakeSociodemographic factors are one of the factors that influence the personal decision to seek health services. M The study conducted in Italy showed that vaccine hesitancy is significantly associated with the economic status of caregivers ranging from OR of 1.34 to 1.59 from low to the severe low economic status of a mother. On the other hand, vaccine refusal was significantly associated with the education status of caregivers, with an OR of 1.89[1.23, 2.93].(19) Similarly, a study conducted in Bangladesh to assess factors that influence full childhood vaccination showed that children born from lower sociodemographic quantile have a lower chance of completing full dose childhood vaccination.(20) Another study conducted in Greece showed that children born from a minority group, those born outside Greece, born from a young mother and had many siblings or their parents were less educated found to be a chance of completing a recommended vaccine according to the vaccination schedule was very less likely. “The weighted proportions of children with complete and age-appropriate vaccination among households with three or more children were 26% and 38% lower, respectively, compared with those of households with only one child.” (21) Another study conducted in Nigeria proved that the sociodemographic status of a caregiver is one of the most influencing factors for optimal childhood vaccine coverage. The study showed that immunization coverage was significantly associated with childbirth order, place of delivery, number of children, maternal age, geographic location, maternal education, religion, literacy level, wealth index, and occupation at a 95% confidence interval in multivariate analysis.(22) The study, which was conducted to analyze factors influencing childhood vaccination coverage, showed that the sociodemographic status of caregivers took the highest share with 35%, followed by antenatal care utilization (17.7%), and maternal education (13.2%), and region.(23) Studies indicated that there is a huge variation in vaccination full coverage across regional states and even from region to Zone and woreda. The study conducted in the Waghimra Zone of the Amhara region showed the percentage of children who are fully vaccinated was higher than the national average but still lower than the World Health Organization (WHO) recommendation. In this study, the most significant sociodemographic factors that contributed to full vaccination coverage were maternal literacy rate, distance from a health facility, and place of delivery (home or health facility).(24) Generally, these studies conducted in the different countries showed that attaining a full course of vaccination according to the country’s immunization schedule remains unachieved, and it also gives a clear impression of how the sociodemographic status of caregiver influences full childhood vaccination. 5.2 Knowledge of caregivers and optimum childhood vaccine uptakeKnowledge is understanding of or information about a subject that you get by experience or study either known by one person or people generally.(25) In the context of this study, knowledge refers to the caregiver’s understanding of or information about vaccine and vaccination, vaccine-preventable disease, and the importance of vaccinating a child for his/her future life that was gained as a result of exposure to vaccine-related information either from a health professional, mass media and house to house volunteer campaign message or IEC materials designed for the purpose of promoting vaccination or informally from a family member, friends, religious leader or traditional leader. Studies showed that mothers’ knowledge about the importance of vaccination is highly correlated with the chance of children being fully vaccinated. A study conducted in Cyprus indicated that mothers with a good knowledge of vaccines were more likely to fully vaccinate their children, and this depended on who is the source of information; trust in the information and advice from a trusted person helped in increasing full vaccine coverage.(26) Improving a mother’s educational status has importance in improving the overall health condition of the family, including children’s vaccination. The study conducted in Nigeria to assess the association between mother knowledge and full vaccination coverage showed that the education status of mothers was highly associated with the chance of their children being fully vaccinated. More significantly, mothers who have an awareness of when to start immunization for their children are more likely to vaccinate their children until they complete the full course of the vaccine according to the immunization schedule of the country.(27)(28) Similarly, a study conducted in Eritrea showed that children born from educated mothers are more likely to be fully vaccinated compared with children born from less-educated mothers.(29) A study conducted in Amhara regional state hard-to-reach areas of Sekota Zuria woreda also showed that mothers’ knowledge of immunization was found to be highly associated with immunization coverage in general.(24) Overall, improving mother education has multiple significant not only on the health of the family but also on the overall development of the country. Hence countries are committed to improving female education enrolment at all levels. This commitment includes the Ethiopian government, which resulted in a significant improvement in female education. Female primary education enrolment improved from 9.4% in 1971 to 96% in 2015.(30) Similarly, through the deployment of Health Extension Workers(HEWs), each woman is getting basic health education, particularly on family health, including EPI, hygiene and sanitation and safe food handling, etc. this intervention basically helped to improve the overall basic health services and helped to improve health-seeking behaviour of the rural community.(31) However, the implementation varies from place to place and depends on the regional and zonal administrative commitment. 5.3 Caregiver’s intention to vaccination and optimum childhood vaccine uptakeThe way caregivers think and feel about vaccines and vaccination influences the decision to vaccinate her/his child. Definitely, a mother with a positive attitude towards vaccines and vaccination will have a high probability of vaccinating her child with full doses. The intention to vaccinate is one of the most decisive factors that affect a decision to vaccinate a child, and a mother needs to break this obstacle before her child gets full childhood vaccination. This will be influenced by individual attitudes towards a vaccine, perceived behavioral control, and the subjective norm. Perceived benefits of the vaccine also determine the chance of vaccinating a child with a full course of the vaccine according to the country’s immunization schedule. In addition, perceived behavioral control is one of the factors that interfere with the intention of the caregiver to vaccinate a child. For example, a mother’s decision to vaccinate her child will largely be determined by the influence of her husband; if a husband has accepted the decision to vaccinate the child, then it is highly likely the child will get vaccinated.(32) Such a kind of challenge to immunization programs is common in Somali, where a mother alone cannot make the decision to vaccinate her child even though the vaccinator went house to house in the absence of her husband. A vaccinator explained the problem in the following sentence: The main challenge we face is taking the vaccine to the house and discovering that the mother and/or child are away. If they are at home, another problem we face is being told that the father is away and that the mother cannot make the vaccination decision. This situation occurred this week during the measles campaign.(33) Similarly, the study conducted in Nigeria, Amibara state, showed that the perception of caregivers is significantly associated with full coverage of childhood vaccination, especially the perception of mothers on the vaccine efficacy, safety, and effectiveness found to be the most influential factors on caregiver decision to vaccinate children.(34) An increase in the knowledge of caregivers about vaccine improves both attitudes and practices on vaccination. Improving the knowledge of caregivers about vaccines cannot be achieved in the short term; these needs coordinated effort and sustainably improved access to information on vaccines and vaccination. Different countries use different strategies to increase caregivers’ knowledge and awareness about vaccines. The studies conducted in Nepal showed that the role of voluntary community health workers was very important in improving caregivers’ knowledge which in return resulted in high vaccination on childhood vaccination.(35) In addition to an awareness creation session targeted to improve the overall knowledge of caregivers on vaccine safety and effectiveness, the role of vaccine promotion using any available means, public opinion, and quality of vaccine service was found to be one of the determinants of attitude toward caregivers and this found to be linked with vaccination coverage.(36) Studies in different countries show that mothers’ positive attitude about vaccines and vaccination was found to be highly associated with the probability of vaccinating their children. A study conducted in the rural setting of western Uganda showed that mothers with better knowledge and awareness of vaccines were found to be more likely to vaccinate their children with full vaccine doses, whereas mothers with low awareness and poor knowledge of vaccines and vaccination were found to have a fear of the side effects and ignore to take their children to vaccination and less likely to vaccinate their children until they complete their vaccination.(37) Similarly, a study conducted in the Amhara region of Wadala woreda showed that a positive attitude about vaccines was significantly associated with vaccinating their children three, two-three times (OR=4.30) and four-five times (OR) 3.227). (38) 5.4 Accessing vaccination service opportunistic cost and optimum childhood vaccinationCosts associated with accessing immunization services are one of the obstacles that affect caregivers from taking their children to the vaccination site. In most cases, the cost includes the cost of administration of a vaccine, which varies from country to country and from public to private facility, and of course, the travel cost of the caregiver to reach the health facility from her/his home. These costs in the US range from around $8 to $29 for administering the vaccine, and assuming a caregiver will cover two hours for travel, it will cost around $23.(39) The cost of accessing the immunization service is not always directly related to the vaccine as the vaccine will be free in most area in the developing world; however, there is an opportunistic cost that affects the decision of caregivers to vaccinate children fully. Comparing children born from a poor family with children born from the richest family, those born from low economic families are 36% less likely to be fully vaccinated at childhood age.(40) There is no proven evidence in the developing country how the cost of traveling hours on foot to get a vaccine will be calculated in terms of money. This remains difficult to calculate, and the feeling will vary from place to place and person to person. In the area where this study will be conducted, the cost of administering a vaccine will be covered by the government, and no cost will be paid by the caregiver. Similarly, transportation costs cannot be calculated easily as a caregiver will walk on foot for hours to reach health facilities. 5.5 Caregiver health facility experience and optimum childhood vaccinationHealth facility experience matters a lot for a caregiver to make another round of visits to get vaccination services. Health facility experience includes caregiver satisfaction with the service provided, health professional communication skills, and missed opportunities. Caregiver satisfaction determines her return visit to the same health facilities; caregivers who are not satisfied with the service will have a low chance of returning for a similar service. A study conducted in Nigeria showed that only 19.4% of mothers who participated in the study were satisfied, while a significant majority (80.3%) were undecided, and 2% of the mothers were dissatisfied with the immunization service provided.(41) A study conducted in Egypt showed that 95% of mothers were satisfied with the immunization service provided at the health center level; however, the satisfaction rate was not associated with full childhood vaccination coverage.(42) Similarly, studies conducted in Ethiopia on the satisfaction of mothers on immunization services showed that a significant number of mothers are not satisfied; only 68.2% of mothers included in the study reported that they were satisfied; however, this study did not mention anything about the association of low vaccination coverage and mother satisfaction with the service.(43) Caregivers’ satisfaction can be affected by different factors, including the health workers’ communication skills. Nowadays, as technology advances, health professionals’ ability to improve communication skills to interact with patients and family members is not improving; health professionals are failing to understand the patient’s biological and psychological problems and empathy to feel their problems and explain how they will be helped. This has a lot of consequences, including a lack of adherence to treatments.(44) Similarly, health professionals understand the challenges of caregivers in obtaining immunization services need to be understood, and they should be helped in a way they will continue to visit the same health facilities. Health professionals’ attitudes towards treating their clients, their technical competency, and their communication skills have a very significant impact on treatment effectiveness, on the client’s knowledge and satisfaction. Similarly, in immunization, health works qualities can be reflected in terms of the coverage and dropout rates, and it will have large consequences at large on the herd immunity (community will be vulnerable to vaccine-preventable diseases).(45) Studies showed that caregivers who met health professionals with good interpersonal communication skills are more satisfied though this area still needs further study; very few health professionals were found trained in interpersonal communication skills in an area where studies were conducted. (46) A missed opportunity is another challenge caregivers face at a health facility who are visiting for immunization service. A missed opportunity refers to an act of caregivers or any eligible person who is eligible for vaccination contacted with health service points and unable to get vaccinated with the intended vaccine type due to several reasons.(47) The missed opportunity is one of the challenges that affect immunization coverage in many counties. Reason for missed opportunities includes the failure of health facilities to administer all vaccines at the same time for eligible children according to the country’s immunization schedule, false contraindication, health professionals’ practice of being unable to open multi-dose vaccine vial for a small number of children to avoid vaccine wastage and logistics problem.(48) The knowledge of health workers to identify contraindication is one of the factors that increases the magnitude of missed opportunities. Studies showed that the knowledge of health workers on contraindication was found to be insufficient or failed to identify it; a study conducted in Burkinafaso showed that 83% of health workers were not able to identify the correct contraindication from the vaccine.(49) Reducing missed opportunities alone will significantly improve vaccination coverage in general and will contribute to getting children fully vaccinated around the globe. Studies showed that reducing missed opportunities alone can improve vaccination coverage in a country by up to 30%.(50) 5.6 Caregivers after service experience and full vaccination coverageCaregivers after service experience like the absence of reminders, health workers unable to explain the common side effect the child may have, cue for action, talking next steps (which of the vaccine the child already received and which vaccine left according to the national EPI schedule), health professional unable to receive caregivers’ feedback about her experience at the point of service etc. will significantly affect the chance of caregiver to do her next visit in the same facility. Evidence showed the more caregivers received balanced information on the benefits of the vaccine and side effects, the more they will be confident to decide on vaccinating their children with a specific vaccine. However, practice from the field showed low to moderate confidence in the vaccine as the amount of information they have remained either limited or not balanced.(51) One of the reasons for missing the schedule for immunization is the educational status of the caregiver and unable to put a reminder about the schedule of the next vaccination. The evidence from Nigeria showed that nearly 90% of caregivers agree that mobile text messages will help to remind vaccination schedule, and they were willing to receive a text message, and about 91% of the respondent said that it would be helpful for them.(27) One means of reminder is to send a mobile text to caregivers regarding the next vaccination schedule, and this was found very important for middle and low-income countries; keeping in mind the timing and repetition of the message affects the decision of the caregiver on taking the child to vaccination site for next schedule.(52) Fear of vaccination side effects is one of the top reasons for caregivers not to vaccinate a child. In addition, inadequate information on the timing, place of vaccination, and the type of vaccine being given has an effect on vaccination coverage.(53) Due to the low staffing in the health sector, it is less likely that health professionals will explain to caregivers about the side effects and next steps during the time of vaccination. This study will carefully observe the practice of frontline health workers on vaccination and their interaction with caregivers. In addition, the previous experience of caregivers will be assessed house to house through structured and unstructured questionnaires to determine how their interaction affected their decision to vaccinate their children fully. 6. Methodology6.1 Study areaThe study area where this study was conducted was located was 254 km northern Addis Ababa, the capital city of Ethiopia. The area is highly marginalized due to a lack of access to an asphalted road that can link to the capital city, and hence supplies that come from other areas are very expensive and not affordable to the local residents. The gravel road that links the area to Addis Ababa is not accessible for small cars all the time, and during summer, it will also be very hard to access the area for long trucks too. The area that can be covered by this study is commonly called the Menz area, which covers about five woredas, namely Menz Lalo, Menz Mama, Menze Gera, Menz Keya, and Menz Gishe. The total population of these five woredas was estimated at around 600,000 though there is no population census conducted to know how many populations exist currently. As far as the researcher’s knowledge is concerned about the study area, though there was an effort to solve the health problem using HEWs, there are still unresolved challenges the community is facing. 6.2 Research approachThis study used both qualitative and quantitative research approaches (Mixed approach). The mixed research approach is used for inquiring information based on the assumption that collecting the diverse type of data provides a complete understanding of a research problem than either quantitative or qualitative data alone. The study began with assessing quantitative information of caregivers that were collected from the sample study participants, which was used to generalize the population; on the other hand, a qualitative study was used to collect detailed information from the study participants to explain the result obtained through the quantitative study. In this study, both qualitative and quantitative data were collected at the same time. The result was analyzed in a similar period separately. The finding was interpreted in the discussion section to compare the finding from the quantitative with the qualitative result.(54) 6.3 Study designResearch design is the conceptual structure within which this research will be conducted; it constitutes the blueprint for the collection, measurement, and analysis of data. This study used a convergent parallel mixed study design to determine factors influencing optimum childhood vaccine uptake in the North Shoa Zone of Ethiopia, particularly in Menz woredas. 6.4 Study populationThe study population was caregivers who are living in five Woredas of the North Shoa zone in Ethiopia. The sample was selected from the study population; caregivers who have children aged between 12-3months of age. 6.5 VariablesA variable in research means simply a person, place, thing, or phenomenon that we are trying to measure in some way.(55) Basically, variables are those factors that affect (facilitate or impede optimum childhood vaccination), which will be measured both qualitatively and quantitatively. These variables include caregivers’ age, educational status, sociodemographic status, knowledge, and awareness about the vaccine, attitude, norm, perceived behavioral control, cost (direct and indirect cost), and caregivers’ pre-and-post health facility experience (during and after immunization service) and vaccine promotion related information. 6.6 SamplingThe sampling technique will follow multi-stage cluster sampling to determine the ultimate sampling units. In this case, this study had considered woredas as a primary sampling unit. The second stage sampling unit was Kebeles of caregivers who were included in the study. The third stage sampling unit, the ultimate sampling unit, is households where caregivers live in. 6.7 Sample size determinationA single proportion formula will be used to determine the quantitative sample of caregivers to be included in the study. Whereas the qualitative sample was taken from the same sample but lower number of caregivers for obtaining more detailed information on similar variables under consideration in this study. Considering the 2018 EDHS result, which shows the national full immunization coverage was 38.5%, the sample calculated was 364 with a margin error of 5% and at a 95% confidence interval. Considering 10% non-response rate, the sample was adjusted to 400. Hence, 400 caregivers were proportionally selected from the total kebeles that were included in the study. Of these study participants selected for the quantitative survey, 20 caregivers were selected for an In-depth Interview (IDI). Detailed information was collected from urban, semi-urban, rural, and remote settings of the study area. 6.8 Data collectionBoth qualitative and quantitative data were collected from January to February 2022. Data collectors were trained for both qualitative and quantitative data collection on the developed tool theoretically and practically before they went to the field to collect actual data. The practical training session was conducted for data collectors on how to use the KoboCollect application besides the questionnaire, and demo data was entered to assess their familiarity with the application. 6.9 Method of data collectionQualitative data was collected using close-ended questionnaires through a trained data collector. On the other hand, qualitative information was collected in open-ended questionnaires prepared to assess factors affecting optimum childhood vaccination according to the caregiver’s journey to immunization, it recommend to use in combination with other data collection. (57) Quantitative data was collected through a house-to-house interview using pre-designed structured questionnaires that were deployed on the KoboCollect mobile-based application, and data was collected using smartphones. At the same time, the qualitative data will use unstructured questionnaires and use both in-depth interviews and observational techniques to collect an in-depth understanding of the situation. In-depth interview: it is a qualitative data collection technique in which one-on-one engagement of participants will take place to explore detailed information about a certain issue. This can be conducted either in person or through a phone interview; the former is a more favorable technique as it will give a better experience of collecting detailed information.(58) The in-depth interview was conducted among selected caregivers using structured interview questionnaires prepared in advance. 6.10 Data processing and analysisBoth qualitative and quantitative data were collected at the same time, and quantitative data was exported from Kobo Collect to MS Excel and then to SPSS version 28. After the data was exported to SPSS, the necessary data cleaning activity was conducted by the researcher. Once data cleaning was completed, the analysis was done starting from basic descriptive statistics and binary logistic regression to determine the degree of association of each variable with the dependent variable. A multivariable logistic regression analysis was done to check which factors have a real association with childhood full vaccination status. On the other hand, qualitative data were collected using open-ended questions, and transcription was ready in Microsoft word document, which later changed to classify according to the theme using Microsoft excel. Each response was coded according to themes, and results were generated for each variable. 6.11 Validity and reliabilityValidity refers to the degree to which the survey measures the right elements that the researcher wants to measure. In a simple term, it means how well the questionnaire can collect the intended response.(60) The data collection tool was checked for validity at different stages. The first stage was to test face validity by asking experts in the area of immunization to rate the questions whether these tools were suitable to collect the intended response or not using the Likert scale (5 to highly suitable to collect the intended response and 1 for inadequate to collect the intended to collect the correct response). The question that got a score of 6 and below from five responses was not considered for collecting data. The reliability of a research tool is the other important factor that the researcher will consider. Reliability refers to the consistency of results; it means the questionnaire will produce the same result being conducted repeatedly under the same condition.(61) Hence, this research work has ensured the reliability of the questionnaire by testing and re-testing questionnaires at different times but same respondents. Testing and re-testing of the questionnaires were conducted in a similar community but which was out of the target population for the final study. 6.12 Ethical considerationEthical consideration is a set of rules and regulation a research activity needs to follow when implementing any study. Ethical consideration guides the research design and practices. The goal of ethical consideration in research is to understand real-life phenomena, study effective treatments, investigate behavior, and improve lives in other ways. Basically, ethical consideration is intended to: Protect the rights of research participants, enhance research validity and maintain scientific integrity. (62) This research activity was conducted maintaining ethical issues as its highest concern area so that the rights of caregivers who participated in this study were protected from any kind of harm or right violation because of their participation in this study. This study has been following all scientific study procedures, including step-by-step Institutional Review Board (IRB) approvals. Before commencing the research interview process, each participant was asked for their consent to participate, and the researcher had explained their full right to participate or not and to withdraw at any time of the process. Each study participant was asked their consent to continue in the interview process. Study participants who complained about the length of the interview and who were not interested finish the process were given the right to do so. During the process of obtaining permission to conduct this study, the Amhara region North Shoa zonal health office and woreda health bureau were communicated about the study’s purpose, and they asked to share the finding by the end of this research process. 6.13 Limitations and delimitation of the studyLimitation: this study is a cross-sectional study where the information was collected at a spot where the data collector contacted caregivers during a house-to-house data collection. This study assumes that caregivers will have a good memory of their health facility experience and able to recall what was their challenges when they travel to health facilities. However, recalling information may depend from person to person and may affect the quality of information obtained. The researcher recommends that future studies focus on an observational study to understand the interaction of caregivers with health facilities and document each process as things happen. This study also used the category of vaccination status, i.e., fully vaccinated and incomplete. However, there is a range of differences even within the categories, like children who received only one dose through outreach vaccination campaigns and children who missed one dose from basic vaccines, which will affect the generalization. Delimitation: this study will focus on factors influencing childhood vaccination only from caregivers’ perspectives in the selected woredas. Due to time and cost, the researcher was not able to include the perspective of others which will remain an area of study for interested researchers in the field. 6.14 Pilot studyA pilot study in research is very important not only to make sure the tools that are going to be used can work to collect the intended information but also to understand whether the overall research approach can work well and the planned budget and time also the right fit for continuing the activity. Research activity is very important, particularly for clinical research. Conducting a pilot study will help the researcher to save time money and increase effectiveness while conducting the large-scale study or the main research activity in the field.(63) A pilot study was conducted in 5% of the study sample in a similar population but not the same study area. 6.15 Result dissemination planThe study result will be communicated to Amhara regional health bureau, zonal health office, and woreda health offices, respectively, to inform the finding and the recommendations the researcher will make by the end of the study. In order to make this practical, the researcher will organize a one-day workshop in coordination with any partner that can support this study, and the finding will be presented to participants. 7. Theoretical FrameworkCompletion of childhood immunization can be influenced by both internal and external factors. This study assessed factors related to caregivers or parents that affect their decision to vaccinate their children. These factors affect the decision-making ability of caregivers and are found at different stages. They are mainly presented in six thematic areas according to the caregiver’s journey to the immunization framework. This study will utilize the caregiver journey to vaccination framework to explore factors influencing the decision-making of caregivers at different stages, both qualitatively and quantitatively. 7.1 Theory of planned behaviorThe theory of planned behavior assumes that individuals act rationally on a certain behavior according to their attitude, subjective norm, and perceived behavior control. It argues that these factors may not necessarily or consciously be considered during decision-making but from the backdrop of the decision-making process. According to this theory, the three factors, either in combination or one of the factors alone, may lead to intention, and the intention will lead to behavior, or each factor alone or in combination may lead directly to behavior change.(64)
Figure 1 Theory of Planned Behavior 7.2 Socioecological modelThe socioecological model broadly sees health as multiple effects of several factors related to individual, family, community, and societal levels. Individual health can be affected by the interaction of a family, community, and society at large. Similarly, caregivers’ decision to vaccinate children will be influenced by different factors starting from individual-level perception to family influence and community-level awareness about the vaccine as well as the overall policy of the government. Hence, the caregiver journey to immunization framework considered utilizing concepts from the socioecological model to understand multiple level factors that influence childhood optimum vaccination status. (65)
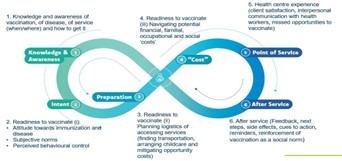
Figure 2: The socio-ecological model 7.3 The caregiver’s journey to the immunization frameworkThe caregiver’s journey to vaccination covers six factors that are related to knowledge and awareness of caregivers towards vaccination and vaccine-preventable disease, her/his intent, ability to decide to take children to the vaccination site and vaccinate the child, household ability to afford to travel to vaccination site, costs associated with taking the child to vaccination site (cost-benefit), caregiver experience at the vaccination site and post-vaccination experience of caregiver and vaccine consequences. These factors are interlinked and explained in the caregiver’s journey to vaccination. The health belief model was a predominant traditional model that explains how certain behavior is practiced and what are the triggering and inhibiting factors. This model was mainly based on the individual past assessment of intention, attitude, and behavior. Considering this limitation, UNICE and other partners developed the caregivers’ journey to immunization framework as a novel way to contextualize and understand caregivers seeking childhood immunization services.(57) This study will explore both qualitatively and quantitively how these factors influence optimal childhood immunization. Experts’ suggestions showed that understanding and improving the caregiver’s journey to immunization would contribute to positive immunization outcomes such as the completion of recommended vaccination schedules, on-time completion of childhood vaccines, and reduced vaccination dropouts.(57) . Figure 3: The Caregiver Journey to Vaccination 8. Result8.1 SociodemographicA total of 404 participants were included in the study, and 371 were willing to stay until the end of the interview session and provide full responses. Out of participants who were willing to give their responses, 298 (80.3%) were female, mainly the mother of the child, 261 (70.4%), and 59(15.9%) of them were the father of the child. The rest of the study participants were grandfathers and grandmothers of the last-born child. Participants included in the study from remote, rural, semi-urban and urban areas. Regarding the educational status of the participants, as shown in the pie chart above, the highest number of 138(37.2%) of the participants were elementary completed, followed by high school complete 111(29.9%) and 90 (24.3%) them were those caregivers who do not have any formal education. The rest segments of the study participants were those who had a higher educational status of degree and diploma 13(3.5%) and 19(5.1%) of the total participants, respectively, and they were living in urban settings. Regarding the occupational status of the study participants, about 244(66%) of them were farmers, followed by merchants who were 44(12%). The rest of them were employees, 34(9%), and other combinations of different businesses were about 41(11%). Significantly, a higher proportion of study participants, 340 (91.6%) of participants’ household annual income fall below 500000 ETB, which is approximately less than $1000 per household. Regarding the religion and ethnic composition of the study participants, all of the participants were Orthodox Christian, and 370 (99.9%) of them were ethnic Amhara. The average distance of health facilities that provide vaccination services was 6.09 km, where the minimum distance was 0.4 km, and the maximum distance was 18km in remote parts of the study areas. Regarding the vaccination status of the last-born child, about 218(59%) of them were fully vaccinated. Table 1: Vaccination status by areas of residence
The vaccination status of children was also found to be affected by caregivers’ educational status. As shown in the table below, children born to caregivers with a diploma and above educational status were found to be more likely to get fully vaccinated as compared with children born from caregivers who do not attend formal education. Table 2: Full Vaccination Status and Caregivers Education
8.2 Association of sociodemographic variables and full vaccination statusVariables like the educational status of the caregivers, area of residency, and distance from the health facility were found to be significantly associated with the full vaccination status of children. Caregivers who did not attend school were found to be 77.1% less likely to fully vaccinate their children compared with their educated counterparts, with a P-value of 0.03. Similarly, children born in rural, remote, rural, and semi-urban areas of the study area were found to have a significant negative relationship with full vaccination status. As shown below in the table, children born in rural and remote areas found to be 77.1% and 76.3% less likely to get fully vaccinated with P-values of less than 0.001. Similarly, children born in semi-urban areas have less chance of being fully vaccinated as compared with children born in urban settings. Generally the sociodemographic characteristics of caregivers affects the vaccination status. Table 3: Association of sociodemographic variables with full vaccination
8.3 Vaccine PromotionVaccine promotion is a way information is communicated in the community, including the source of information, the credibility of the information, and adequacy of the information to the extent it can help the community members be convinced to vaccinate their children. 8.3.1 Source of informationThis study indicated that the main source of information about vaccines is health professionals/ Health Extension Workers (HEWs). From a total of responses, 280 (72.4%) of them get information through HEWs house to house information dissemination, followed by kebele leader 92(23.8%). Other sources of information like TV/radio, friends, and social media seems among the least utilized source of information. Similarly, HEWs were the most trusted source of information about vaccines in the community, followed by Kebele leaders. 8.3.2 Caregivers’ opinions about vaccine promotionOut of the total study participants, 267(72.3%) of them agreed that the way vaccines had been promoted in their communities was enough to motivate caregivers to vaccinate their children. In the meantime, a significant number of them believe that the vaccine promotion in their community was not adequate for informing caregivers about vaccinating their children. https://irpj.euclid.int/wp-admin/upload.php https://irpj.euclid.int/wp-admin/upload.php Table 4: Caregivers’ opinions about vaccine promotion in their communities
8.3.3 Qualitative data result [in-depth interview] about vaccine promotionThe qualitative study showed that most of the vaccine promotion, including the time of vaccination (vaccination schedule) mainly done through health professionals (HEWs) and Keble leaders. Most of the caregivers agree on the adequacy of vaccine promotion done in their community, while few of them reported that they did not get adequate information about the vaccines. A caregiver from Yigem Kola Keble 05 respondent’s ID 003 stated her experience regarding vaccines promotion in her community. Well, there is vaccine promotion. Most of the time, health professionals do it. Sometimes, the kebele leader will call on the phone and tell on the presence of vaccination and the date of vaccination. We got additional information from health professionals on the benefits of vaccines during our visit to the health facility. They told us the type of disease vaccine could prevent and the need for continuing routine immunization monthly. 8.3.4 Association of vaccine promotion and full childhood vaccination statusThere was no significant association found between the full vaccination status of children and vaccine source of information and the opinion of caregivers about the adequacy of vaccine promotion. However, the qualitative information showed that vaccine promotion had contributed a lot to starting vaccines on time. 8.4 Knowledge and awareness about vaccineOut of a total of 371 respondents, about 338 (91.1%) of them thought that childhood vaccination could help to prevent disease. Caregivers were asked to mention the type of diseases that vaccines can help to prevent, and a significant majority, 234 (63.07%), of them mentioned measles, followed by tetanus, 135 (36.39%), and polio, 39 (10.51%). Other different diseases like diarrhoea, night blindness, headache, common cold etc., sum up to give the rest majority. At the same time, other important diseases like TB, HPV, Hep, and pneumonia were found to be the least known by the caregivers. In an area where this study was conducted, a significant majority of them, 265(71.4%), give birth at home and miss the first vaccination like polio 0. In addition, they did not know when to start vaccination and complete it. A majority of caregivers, 242(65.2%), did not know when to start vaccination for their children and when they could complete it. The vaccination status of children was determined through vaccination card observation by data collectors and through an interview of caregivers regarding their status in cases where vaccination cards are misplaced. During the data collection period, only 217 (58.5%) of the caregivers have the vaccination card. Out of the total study participants, 239(64.4%) of them had an awareness of vaccine side effects. The most commonly mentioned side effects were fever 181(50.7%), swelling 126 (35.29%), and local pain 70(19.61%). The majority of them, 225(63.03%), had an awareness of what action was needed in cases of vaccine side effects. Though a significant majority of the total respondents, 89.08% of them, know where they can get childhood vaccination, still there are a few respondents who do not know where they can get vaccines. Most of these respondents were those who live in remote and rural parts of the study area. About 349(94%) of caregivers who participated in this study agree that vaccination is important for the health of children. Similarly, 346 (93.26%) of the total respondents agree that all children should get fully vaccinated to be protected from diseases. 8.4.1 Qualitative data results (In-depth interview) about the Knowledge and Awareness of VaccinesQualitative data was collected from two towns, semi-urban areas, and rural and remote kebeles of the study area. In-depth interviews on the knowledge of the caregivers about full childhood vaccination are summarized in the following way. Table 5: Description of caregivers’ response on on vaccine knowledge
8.4.2 Benefits of vaccinesMost of the caregivers know the benefits of vaccines; regardless of the expression, they say vaccines are important for the better future of children. They think childhood vaccination helps children grow healthy and strong. They understood the benefits of childhood vaccines for the family as well. The majority of them said childhood vaccines help family members by avoiding unnecessary stresses when children get sick. A respondent from Molale town with an interview ID of 015 stated the benefits of the vaccine in the following way: Well, vaccines are very important in many ways; children who get the vaccine will be healthy. Vaccines prevent different diseases like measles, smallpox, tetanus, and other diseases… even they can prevent disabilities. It also helps to make the bone strong. Overall, the vaccine helps children to grow healthy and strong. I usually hear about vaccines’ benefits from health workers and radio. Another respondent from rural kebele of Menz mama Emegua kebele with a respondent ID of 011 stated the benefits of vaccines as follows: “vaccines are key to prevent disease outbreak (ተስቦ-Teasibo) and anyone vaccinated can be prevented from the disease easily.” On the other hand, there are caregivers who do not have a good understanding of the benefits of vaccines. They think vaccines are not as relevant to the health of the child and think sometimes vaccines may cause serious complications. There are caregivers who gave a response during this study who said vaccines themselves might kill the child. Respondents with an interview ID of 05 from Kewariat Keble stated their understanding of vaccines in the following way. I think it will not be bad for children if they are not vaccinated. I do not think unvaccinated children will develop the disease. Instead, vaccinated children will develop the disease. They will develop diseases when they had injected with the vaccines. This cause problem for the family and the child. I prefer not to vaccinate my child. Most of caregivers share similar ideas on the type of disease childhood vaccines can prevent. They said childhood vaccines could prevent diseases like measles, polio, and flu. If vaccinated, children will be protected from these kinds of diseases. This research showed that there were also misperceptions of vaccines’ benefits, like children playing on dirty playing fields can be protected from being sick because they are vaccinated. Caregivers were also asked about the benefits of fully vaccinating children. Most caregivers believe that fully vaccinating will help children to get full protection from diseases. They believe that partial vaccination is partial protection. A respondent ID 002 from Kolo Margefia stated that “well, the benefits of fully vaccinating children is to help them being protected from many diseases. One vaccine cannot prevent all types of diseases. If the child is fully vaccinated, then he will be protected from many diseases.” 8.4.3 Consequences of unvaccinated childrenMost of caregivers believe that unvaccinated children will face problems. They also expressed the burden on families, including financial and psychological burdens as a result of children’s sickness that could be prevented by vaccination. The response from a caregiver with a participant ID 017 stated as follows: The unvaccinated children will face many problems; they may develop a disease like measles, polio and flues, and tetanus. Children who suffer from disease will not grow healthy. There is also a consequence on the family. When children get sick, we will be stressed, and this is not good for the whole family. The other caregiver from Molale town 01 Keble with a respondent ID 12 indicated that an unvaccinated child would cause a burden for the entire family. The caregiver believes that an unvaccinated child may be a reason for disease transmission in the community. She said, “the unvaccinated child will cause disease for other children in the family. The child who is not vaccinated will develop disease first, and it can transmit to other healthy children.” On the other hand, caregivers who were not aware of vaccines’ benefits believe that there is no consequence of being unvaccinated. They believe vaccines themselves will cause a burden to children due to their unpleasant effects after vaccination like fever, pain at the point of vaccination, and sometimes more complications, according to their thought. 8.4.4 Association of caregivers’ knowledge and awareness and full vaccination statusThe caregivers’ knowledge about when to start the vaccination, complete it, and their awareness about the place where vaccination will be given was found to be significantly associated with the full vaccination status of children. Caregivers who know when to start vaccination and when to complete it were found 9.22[5.15, 16.49] times highly likely to fully vaccinate their children during childhood with a P-value of less than 0.001 at 95% CI. Likewise, caregivers who know where to get vaccines were found to be 7.72[2.72, 12.02] times more likely to fully vaccinate children with childhood vaccines. 8.5 Decision making and process of getting the vaccinationThere are different steps caregivers need to pass through to get their children vaccinated. This begins with a motivation to decide on vaccinating a child, and that usually comes from a close family member. For most of the caregivers, encouragement comes primarily from their spouse 204(54.9%), followed by other family members 147(39.5%), 112(30.25%) HEWs, and kebele leaders 37(10%), respectively. The majority of decision-makers on vaccinating a child were found to be caregivers themselves. Generally, the overall attitude of the communities about the vaccine was found to be encouraging. About 345 (92.99%) caregivers responded that the community attitude about vaccination is encouraging. Friends were found to be one of the highest proportions in terms of discouraging vaccination, followed by mothers and other community members. Once the caregiver decides to vaccinate, the next challenge is arranging transportation to the vaccination site. Regardless of the distance between the health facility and the house of caregivers, most of them, 345(93%), travel on foot to get vaccination services. About 37(10%) of the total respondents need to travel on foot more than 8km, with a maximum of 18km, to get their children vaccinated. Once after, the caregivers manage to arrive at health facilities where vaccination services will be provided; their chance of getting their children vaccinated will be determined by other factors like the availability of vaccines and getting the health facility open. About 255(68.7%) of them can get the vaccine without any difficulties in health facilities any time they visit. At the same time, a significant number of caregivers have a challenge accessing vaccines when they attempt to vaccinate their children, including health facilities permanently closed in their areas. Table 6: Experience of caregivers to access vaccines when they visit health facilities
Another challenge for caregivers to get vaccinated their children were the presence of competing priority. Caregivers should make sure children and other family members, as well as the entire household, need to be handled carefully in their absence. Hence, especially mothers need to assign someone who can take care of the rest of the children and the household before heading to a health facility. In the means time, it is not an easy task to get someone to assign who can handle this responsibility. More than 234 (63%) of the study participants indicated that it was not easy to assign someone when they went away for vaccination. Table 7: Caregivers’ experience of getting someone who can take care of their house when they travel to the health facility.
Usually, caregivers will be scheduled on a certain day to visit the health facility; however, that day may not be convenient for them to visit health facilities. For example, they may face a problem that requires social responsibilities like attending funeral ceremonies, where caregivers should attend or must delegate someone. caregivers were asked to mention some of the obstacles that prevent them from visiting health facilities and consequently lead to being unable to vaccinate their children fully. Even though the majority, 251(67.65%) of them, indicated that there is no such problem with visiting health facilitie, at the same time important portion of caregivers still faces many challenges in vaccinating their children. In this study, caregivers reported that forgetting the vaccination schedule was not a common problem. About 320(86.3%) of them reported that they could not forget their vaccination appointment. For the question, caregivers asked what they would do if they forgot their schedule; nearly half of them, 199(53.6%), responded that they would immediately take their children to the health facility. In the meantime, a significant proportion of caregivers, 79(21.3%), did not know what to do. 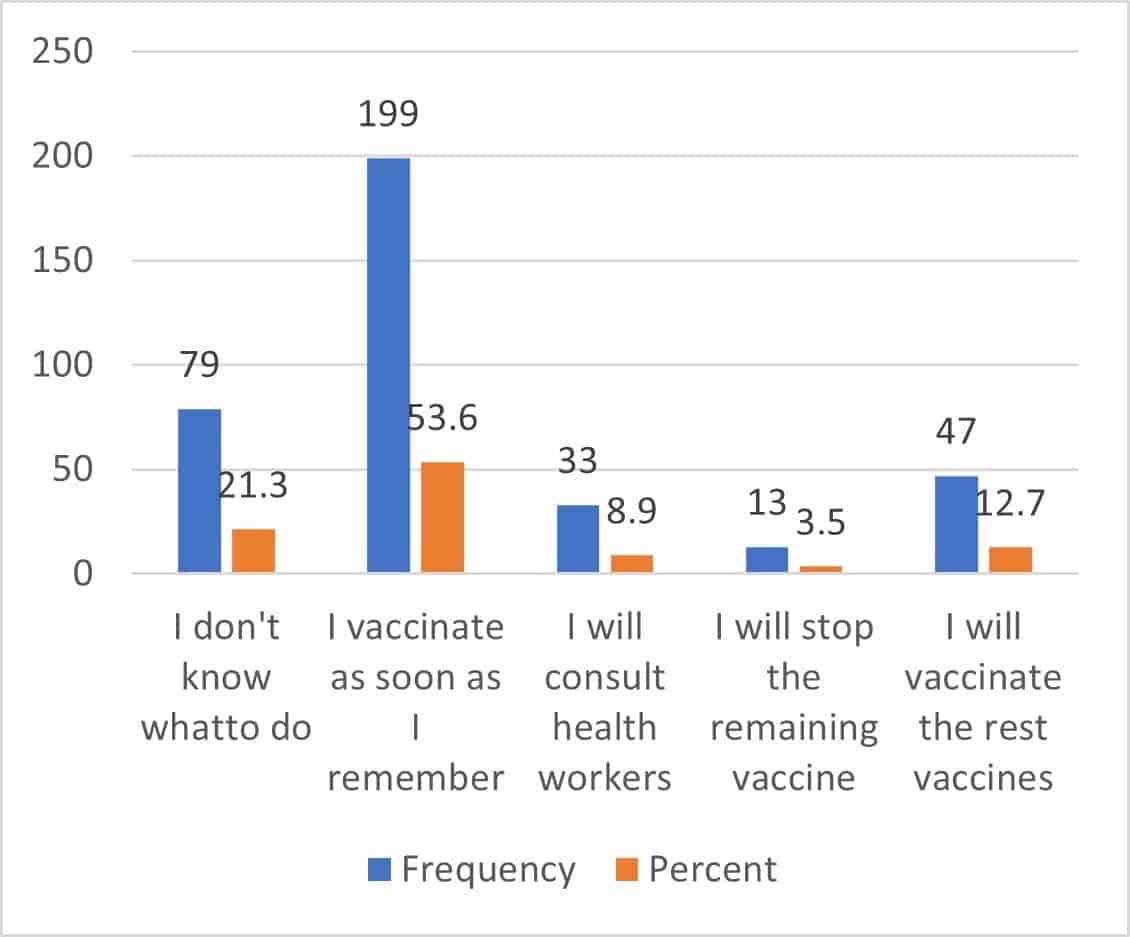 https://irpj.euclid.int/wp-admin/upload.php Figure 4 : Caregivers’ response on actions they will take if they forget their vaccination schedule As caregivers will have so many responsibilities, and while they focus on their household activities, chances are high to forget their vaccination schedule. There are different means to remember vaccination schedules, about 169(45.6%) of caregivers use their personal reminders, while 127(34.2%) of them were helped by HEWs to remember their vaccination schedule. About 32(8.6%) of them did nothing to remind the vaccination schedule. 8.5.1 Qualitative data finding [In-depth interview] on the decision-making and process of vaccinationQualitative data on the decision-making and process of vaccination findings showed that there are different actors involved in decision-making and challenges that encounter the process of vaccination.
Table 8: Description of caregivers’ response on vaccination decision making process
8.5.2 Decision-making on vaccinating a childThe finding showed that mainly the mother and father of the child are the primary decision-makers in the process of vaccinating a child. Others like the grandmother of the child and friends also play a significant role in deciding to vaccinate a child. A caregiver from Molale town, age 30, with the respondent ID of 012, has stated her preparation in the process of vaccination as follows: Normally it is my husband and me who can decide to vaccinate our child. Sometimes my mother will decide to vaccinate or not. There is no complicated process of decision-making to vaccinate my child. For the first time, I took my child to the vaccination center 45 days after I gave birth and then after I took him every month. For the last vaccine, they scheduled us to come in the ninth month. Another caregiver, the father of a child from Molale town, stated that: Deciding when to vaccinate the child is not complicated; everybody vaccinates their children here in Molale town. You take your child to the health center, and then they will vaccinate him. Usually, it is my wife and me who decide when to vaccinate the child. For the first two rounds of vaccination, my mother used to go to the health center with my wife; then, after, my wife went alone until the child finished his vaccination. From the expression of caregivers, we can learn that there is some misunderstanding on the timing of vaccination and the process of vaccination. A caregiver from Yigem Kola Kebele with a respondent ID 003 described the process of vaccination and his understanding in the following way: Well, I think there is no need for preparation. What is needed is just being careful and waiting for the monthly schedule and taking the child to the health post. I believe the vaccine will cause illness to the child, but that is temporary; it will not be long-term and will not cause serious illness. I believe children should be vaccinated every month until the age of five years. 8.5.3 Preparation for vaccinationRegarding the means of travel and how they start their journey to the health facilities; a caregiver from the Molale with respondents code 017 stated that: When I decide to travel to the health facility, first I will clean my child, change her cloth, and travel to the health center; that is all. No one can take care of my house, so I will lock my house when I travel to health facilities. If I get the three-wheel vehicle (BAJAJ), that will be fine, I take one, and I will travel. If there is no transport from my area, I travel on foot; it is not far from here, and it will take me about 30 minutes to reach the health facility. Another respondent from Kolo Margefia Kebele stated what steps she would take before traveling to the vaccination site. When health professionals inform us that the vaccine vials are open, then we will take our children to the health facility to vaccinate. I cannot get anyone to look after my house; therefore, I lock my house and travel to the vaccination site. I perform all of my household activities after I return from the health center. Sometimes, there will be a long queue, and I stay in the health center a long time before I get my child vaccinated. The health facility is not far from my house. I can travel on foot. There is no transportation from my house to the health facility. Another caregiver from Emegua Kebele with a respondent code 001 started the process of getting vaccination in their kebeles as follows: Since I do not have anyone who can take care of my house and my family, I have to prepare everything one day before the vaccination day. I prepare food and all other household activities before traveling to get my child vaccinated. The process is not complicated. We travel on foot from home to the health facility. It takes about 1:20 hours to reach the health facilities. Generally, health workers are good. They gave vaccines to our children, and they also educated us on the vaccination schedule. But I have heard some of them are not good at vaccinating children; the way they handle the needle cause pain to the child, and they use force to inject the vaccine. Regarding the queue, it usually takes 1 hour to wait, but sometimes it may take half a day, and I may have to wait in the afternoon to get the vaccine. Overall, it takes one full day to vaccinate a child. 8.5.1 Association of decision making and process of vaccination variables with full vaccination status Among variables that affect decision making and hinder the process of vaccination, encouragement of other people to the caregivers to vaccinate their children, availability of vaccination service in the health facility, household activities, forgetting vaccination schedule, and reminders to vaccination schedule found to be significantly associated with fully vaccinating childhood vaccines. The study indicated that caregivers who have an encouraging spouse, family members, and HEWs were generally more likely to vaccinate their children fully. Caregivers who had encouraging husbands were found to be 9.87[3.84, 25,36] times more likely to fully vaccinate their children with a p-value less than 0.001 at 95% CI. Caregivers who did not get vaccines in most of their last visits were found to be 90% less likely to fully vaccinate their children, with a P-value of less than 0.001 at 95% CI. Another factor that affects the likelihood of vaccinating children is the household-level activities of caregivers. The finding from this survey showed that caregivers who could get someone easily to delegate for household activities were 3.4[1.62,7.14] times highly likely to fully vaccinate their children with a P-value of 0.001 at 95% CI. Remembering the vaccination schedule was also found to be significantly associated with complete vaccination status. This study showed that caregivers who can easily recall their vaccination schedule were found to be 2.28[1.25, 4.17] times more likely to fully vaccinate their children, with a P-value of 0.007 at 95% CI. Caregivers who put their own reminder to remember their vaccination schedule was 2.42[1.22, 4.79] times more likely to vaccinate their children, with a P-value of 0.01. On the other hand, caregivers who did nothing to remember their vaccination schedule were 90% less likely to vaccinate their children, with a P-value of 0.001. Table 9: Association of decision-making and vaccination process-related variables with full vaccination status
8.6 Caregivers’ pre- and post-vaccination health facility experienceCaregivers’ health facility experience is an important factor that influences the chance of re-visiting the same facility for vaccination service. The study showed that the interaction of the majority of caregivers with the health facility was good, with the exception of a few responses collected: one caregiver reported as very bad, two responses as bad, and the other 30 responses as neutral; the rest of the study participants indicated that their health facility visit was either good or very good. Regarding the interaction of caregivers with a health professional during a health facility visit, the study showed that there was a gap; only 198(53.4%) of them can easily discuss any possible side effects after vaccination and seek advice. The majority of caregivers, 314(84.6%), reported that reception in the health facility was good. Caregivers were asked to share their experience of hearing other caregivers complain about health facility experience. The study showed that the majority of them, 264(71.16%), did not hear any complaints, while the rest, 101(27.22%), heard and the others did not remember. Feedback play a great role for improving services; majority of caregivers, 256(69%), were not asked for feedback about the vaccination service. Similarly, only 182(50.8%) of caregivers were informed by health professionals on the type of vaccine the child was given, while the other half of this study participants were not told the type of vaccine their child got vaccinated or very rarely, they have been told. On the other hand, this study showed that 324(87.3%) of caregivers were informed of the next vaccination schedule, while the remaining 47(12.7%) were not told when to re-visit the health facility for vaccination service. This study found caregivers who returned without receiving vaccines after hours of foot walk to get vaccines; 88(23.7%) experienced a return before getting the vaccine due to several reasons like absence of a vaccine, health facility closure, or absence of HEWs in the health facility. About 24(65%) of the total caregivers experienced closed health facilities. Out of these caregivers, 6 of them never visited a health facility after that day, and their children dropped their vaccination; 16 of them returned another day for the same service; and 2 of them went to another health facility on the same day and vaccinated their children. Explaining common vaccine side effects and AEFI to caregivers during the time of vaccination plays a significant role in reducing the number of vaccine defaulters. However, this study showed that more than half of the study participants, 191(51.5%), were not told about vaccine side effects. Consequently, the significant proposition of caregivers, 129(34.8%) do nothing when their children experience vaccine side effects. This research showed that, of total study participants whose children experienced vaccine side effects, 52(14%) of them dropped the next vaccines. Caregivers were asked to respond on the overall quality of vaccination service provided to them; the majority of them were satisfied with the service, 148(39.9%) said the service was very good, and 144(38.8%) of them said the service was good. On the other hand, 11(3%) said the service quality was very low, 14(3.8%) reported low, and the remaining as a medium.
Figure 5: Caregivers’ response to the overall quality of vaccination service provided for them Caregivers were also asked whether they could recommend the same health facility for immunization service, and a significant proportion, 105(28.3%), of them, reported that they would not recommend it to others. 8.7 Qualitative study result [In-depth interview] about caregivers’ experience in health facilitiesMost of caregivers interaction with health professiona was good; they reported that health professionals were respectful and encouraging, and they gave them advice on continuing vaccination. In the mean time there were caregivers who complained about the long queue. A caregiver from Meleya Kebele 07 with respondent code 017 stated her experience with the health facility as follows: My experience in the health facility was very good. There was nothing that I did not like. The health professional (HEWs) was very good. Sometimes she comes to my home and vaccinates my children. Another caregiver from Molale 01 Kebele with a respondent ID 012 stated her experience of visiting the health facilities for vaccination services; she described her experience in the following way: hmm, there is no such interesting thing I saw during my visit; for me, it was not good. Especially since they were changing nurses regularly, we met new nurses and those nurses were also with bad temper/behavior. The nurse said, ‘we cannot open vaccine vials for a few children, wait, and we will open.’ These and other experiences were not good for me. Most of the caregivers complain about the services being provided, I heard some of them saying, ‘when do we have a better service?’ I had seen some of them leaving the health facility, saying I will never come back to this facility. Another caregiver from the same kebele with respondent code 017 had a different experience of a health facility visit. But they share a common problem that was unable to open vaccine vials for a few numbers of children. This caregiver stated her experience in the health facility as follows: She also added here a recommendation for the future to improve the vaccination service and help caregivers complete their vaccination: I think the government should make vaccines available; if vaccines are available, then health professionals will vaccinate children without a problem. Vaccines are important for the health of children, and we all agree on this. Another thing, the government should assign more nurses to the health facility to avoid the long queues to get vaccines. Waiting long queue is discouraging for caregivers. One last thing about health professionals, they should not say, ‘we cannot open a vaccine vial for a few children’ any children who come to the health facility should not leave the facility before getting the vaccine. Another caregiver (father of a child) from Yigem Kola 05 kebele code 003 describes his experience as follows: If we miss our vaccination schedule, there is mistreatment and discomfort. On top of this, the child got sick after the vaccine, and she was crying. Sometimes the HEWs come to the health post very late, causing a long queue and long waiting time. Overall, it is good. Having all these discomforts, including very long distances travel, still, it is fine to get a vaccine because the health of our child is above everything; we can tolerate everything to get the vaccine. But for the future, I think it will be good if they arrange more vaccinators to reduce the long waiting time. Well, regarding experience sharing with another caregiver, yes, we have been chatting and discussing many things, including vaccination itself. I have heard others complaining; some said, ‘oh, it could have been nice that I did not come here. Next time I will not come here; when we hear such things, we say to ourselves, oh, there is something worse than us, and we stop complaining. 8.7.1 Caregivers’ post-vaccination experience [In-depth interview]Caregivers described their experience after vaccination service. Most of them received advice from their health professional on the next vaccination schedule. Upon their arrival in their village, most of them were asked by their community member where they were coming from, and caregivers explained their journey. Most of them described that they had experienced minor side effects of the vaccine-like fever and pain at the point of vaccination. Some others described the Adverse Event Following Immunization (AEFI) as a change in behavior of a child because children will cry for a long time that day and the next day. A caregiver from Molale 01 Kebele with a respondent ID 012 described her post-vaccination experience in the following way. After vaccination, my child experienced fever; it was only fever and small swelling on the site of vaccination, and the next day, he started to feel good. But, for the first time, I was very worried that he would be sick; he was also crying for a long time, and he had never had that kind of behavior before vaccination. Yes, when I came back from vaccination, my friends and a family member had asked me about my experience, like who was today’s doctor, is he able to vaccinate the child carefully? did he put the needle slowly?, or what did he do?; questions like that. My experience with the health facility was almost similar. There was a similar queue that I had to wait for before getting the vaccines. Another caregiver from Yigem Kola Keble 05 respondent ID described her post-vaccination experience as follows: Well, besides household activities being mismanaged, there were other challenges like our cows and oxen may feed on dirty water, Leeches[አልቅት] that cause them to be sick and even die. There are many challenges that affect your life when you leave your house without someone that can protect your property. After the vaccination program, no one had asked me a question. The vaccination service is the same as it used to be; no changes have been seen. Of course, they told me the next vaccination schedule before I left the health facility. Besides, they put a scheduled date on the vaccination card, and I refer that to return to the health facility for the next vaccination. The Keble leader also reminds the vaccination day in advance. Yes, our children had experienced sickness after vaccination; he had a fever, swelling and pain at the point of vaccination, and diarrhea. We massaged his hand with Vaseline and left it; then, he started to feel good. Another caregiver from Kewariat Kebele 06 respondent ID 005 stated his response about his post-vaccination experience. We did not go to health facilities for vaccination. Sometimes the health professional comes home to home, and they vaccinate our children. I do not remember any questions asked by health professionals about the vaccine. Whatever they said, I trust in God, I firmly believe in God, and I left my entire life for him. However, if you are forcing us to vaccinate, we will vaccinate, but I do not believe the vaccine is important. … Since I never went to the health facility, I do not have any experience with what you are asking me. Another caregiver from Kolomargefia Kebele 017 respondents ID 002 stated her post-vaccination experience in the following way: The vaccination site was not far, and I went there and got the vaccine, but after I returned home, my child was sick; he was crying, and there was time for him to feel very painful, and he continued crying. At one time, because my child was very sick, my husband said to me, ‘never go back to this health facility.’ Because he thinks the pain was caused by the vaccine itself. The service in the health facility has been improved from time to time. However, there is still fear among community members regarding vaccination. Some of them also experienced the same problem as me; when we talked in the health facility while waiting for the vaccine, they told me that their children got serious illnesses from the previous vaccination. Some others said their child is losing weight after getting vaccinated. 8.7.2 Association of decision-making and vaccination process-related variables with full vaccination status of childhood vaccines There are variables that are significantly associated with full vaccination status like caregivers’ interaction with health professionals at a health facility, their exposure to other caregivers complaining about vaccination service being provided in the health facility, feedback asked, informing on the type of vaccine given to the child, communication of the next vaccination schedule etc. the table below describes the association of variables. Table 10: Association of decision making and process of vaccination with full vaccination status of childhood vaccines
8.8 Variables which have a significant association with full vaccination status (multivariable regression table)Following a bivariate analysis, a multivariable logistic regression analysis was done to show the variable which has a true association with the dependent variable. Accordingly, the result showed that caregivers do not have an awareness of where to get the vaccination AOR 0.33[0.12, 0.9] with a p-value of 0.003, and when to start vaccination AOR 0.23[0.11, 0.47] with a p-value <0.001 at 95% CI. This shows caregivers who did not know where to get vaccines were 67% less likely to vaccinate their children fully, with a p-value of 0.003. similarly, caregivers who did not know when to start vaccination were 76% less likely to fully vaccinate their children. On the other hand, distance from the health facility was found to be one of the significant factors that had affected full vaccination status in the study area. The study showed that caregivers who travel 1-4 km and 5-8 km were 80% and 76% less likely to fully vaccinate their children, with a p-value of 0.003 and 0.01, respectively. Caregivers’ decision to fully vaccinate their children was found to be affected by their peers. This study showed that caregivers who heard complaints from other caregivers found 67% less likely to fully vaccinate their children, with a p-value of 0.003. Health professionals’ role in advising caregivers on the next vaccination schedule was very significant to help them return for vaccination. This study showed that caregivers who did not receive any advice from health professionals regarding the next vaccination schedule were 65% less likely to fully vaccinate their children, with a p-value of 0.048. This study showed that vaccine promotion in the study area was not adequate, and it is based on interpersonal communication by HEWs. This study showed that caregivers who strongly disagree with the adequacy of vaccine promotion were found to be 79% less likely to fully vaccinate their children, with a p-value of 0.029. on the other hand, forgetting the vaccination schedule remains an important factor. Caregivers who can recall their next vaccination schedule without any difficulty were found 7.46 times more likely to fully vaccinate their children with a p-value of <0.001. see the table below for multi-variable regression results. 9) DiscussionThis study used both qualitative and quantitative techniques to explore information on factors influencing childhood vaccination in the study areas. The study explored factors related to the sociodemographic characteristics of caregivers, knowledge, and awareness about vaccines and vaccination, decision making and process of vaccination-related factors, and caregivers’ experience in health facilities. The finding showed that about 218(59%) of children were found to be fully vaccinated, which shows the vaccination status of the area is not yet optimal; it is far from the recommended coverage, 90% according to the World Health Organization. The finding showed that the coverage is slightly better than the national average, and the study findings which was conducted in eastern Ethiopia.(69) Nevertheless, it remains one of the lowest compared with the WHO recommendation.(70) 9.1 sociodemographic factors and optimum childhood vaccine uptakeThe sociodemographic factors are those that contribute to the general well-being of a given society, and when it comes to the health of individuals, these factors play a significant role. Children born from a wealthy family have a high chance of being fully vaccinated, while children born from a family of low economic status will have less chance of being fully vaccinated. (19) Similarly, this study showed that children born from low economic status have a low chance of being fully vaccinated. Caregivers who participated in this study have an almost similar economic situation which is less than $1000 annual household income, and the economic situation may not be the right factor that differentiates one caregiver from other. Keeping the economic situation the same, other factors like caregivers’ education status, distance from the health facility, and residential area were found to be significantly associated with a childhood full vaccination status of children. The finding from this study also agrees with previous studies conducted in Nigeria(71) and Mozambique.(72) On top of the low economic situation, which applies to almost all caregivers who participated in this study, those who had good educational status, lived near to a health facility (in less than a 2-kilometer distance), and those living in an urban setting has more likely to get vaccinated their children than their peers with the opposite. Comparing caregivers with their educational status of degree or diploma, those who do not get formal education were found to be 70% less likely to vaccinate their children. The influence of educational status on vaccination seems until high school and no difference is seen between caregivers who completed high school and degree holders in terms of its association with full vaccination status of children. Similarly, comparing caregivers living in town with those living in rural and remote areas were found to be 71% and 78% less likely to vaccinate their children until they complete their childhood vaccine. A similar study conducted in different countries agrees with the findings in this study; a study from Ghana showed that children born in rural areas were 55% less likely to get fully vaccinated. (73) Similarly, previous studies conducted in Ethiopia showed that children born in rural areas were 60% less likely to get fully vaccinated.(74) The qualitative study findings also have complimented the effect of sociodemographic characteristics on the full vaccination status of childhood vaccines. A caregiver from Goch Kebele with a respondent ID 007 and got no formal education stated her perception about vaccines as follows. “You know I am not an educated woman; I do not understand what the health professional some time ago told me about this thing. I never attempted to vaccinate my child unless they came and vaccinated my child. The health post is very far from here.” This signifies the importance of caregivers’ educational status, and distance from health facilities can affect childhood vaccination status. In the multivariable logistic regression, one of the factors found significantly associated with full childhood vaccination status was a distance from the health facility, and it showed caregivers who are living 1-4 kilometers away from the health facility found to be 80% less likely to fully vaccinate their children and similarly caregivers who are living 5-8 kilometers away found to be 76% less likely to fully vaccinate their children. This study showed that nine kilometers and above distance was found to be not associated with full vaccination status. However, since very few caregivers were found to be included in the study who need to travel more than 9 kilometers to get vaccination service, this study cannot conclude the evidence can be generalized. Looking at a response from the qualitative study, we can understand the role of sociodemographic variables on the vaccination status of children in the study area. Those children born in the town, from an educated family, and with better economic status were found to be highly likely to be fully vaccinated for their childhood vaccines. At the same time, those born in rural and remote areas were found to be less likely to get fully vaccinated. Their chance of being fully vaccinated is further deterred by other factors like the influence of family and community members. Generally, this study showed that childhood full vaccination status was found to be significantly associated with sociodemographic variables like caregivers’ education status, distance from a health facility, and residential area (Urban and other like remote, rural, and semi-urban). 9.2 Knowledge and awareness of caregivers and optimum childhood vaccine uptakeCaregivers’ knowledge and awareness about the vaccine is one of the most important factors that determine the chance of children being fully vaccinated on childhood vaccines. This will be influenced by the availability of information to the people from a trusted and reliable source that ensure vaccines are relevant for the health of children and their growth and future wellbeing. This study assessed the source of information about vaccines for each caregiver, and the finding showed that nearly all caregivers get information about vaccines through interpersonal communication. The majority of them, 72.4%, got information about the vaccine from health professionals (HEWs), while the remaining got information from kebele leaders. The qualitative information also supported this finding; caregivers trust information about vaccines when they hear it from health professionals. Caregivers think health professionals are accountable for their word. A caregiver from Yigem Kola Kebele 05 respondent ID 005 stated his belief about the source of information in the following way: Well, health professionals are not accessible most of the time, but when they are accessible, they are my trusted source of information. Kebele leaders also promote vaccines, and he told us information about vaccines, but we trust health professionals, we do not trust others, we say he is not a health professional, and we think he may not have knowledge about vaccines. A bivariate analysis was conducted to show the significance of the trusted source of information and full childhood vaccination status; this was not significantly associated. As the finding showed, almost all caregivers trust information from health professionals and very few from other sources like TV and radio. The adequacy of information on vaccines is one of the most important factors that play a significant role in terms of improving vaccination coverage in a certain area. The study finding showed that a significant majority of them at least heard about vaccines either from health professionals or Keble leaders. However, as shown by this study, a significant number of caregivers were not received important information about the vaccine: when to start the vaccine and where to get the vaccine. A significant proportion of caregivers also believe that vaccine promotion is not adequate in their locality, and this was found to be significantly associated with full childhood vaccination status with AOR 0.21[0.05,0.86] with a p-value of 0.029 at 95% CI. This study finding agrees with other studies conducted on the importance of vaccine promotion to increase childhood vaccination.(75) When we see the knowledge of caregivers, a significant majority of them, 91.1% of caregivers who participated in this study, knew that childhood vaccination could prevent at least one kind of disease. However, since the majority of them, 71.4%, gave birth at home, consequently they missed the vaccine at birth. The previous study also showed how health facility delivery and childhood vaccination coverage are interlinked.(76)&(77) Moreover, the majority (63.07%) of them did not know when to start vaccination where they could have been informed at the time of birth in a health facility. This shows there is a high need to improve health facility delivery to enable caregivers to start the vaccine as early as birth. On the other hand, a significant number of caregivers did not know where they could get vaccines, and this was found to be significantly associated with the full vaccination status of children, AOR 0.33[0.12, 0.9] with a p-value of 0.03. Similarly, caregivers who do not know when to start vaccination were found to be 77% less likely to vaccinate their children fully, AOR 0.23[0.11,0.47] with a p-value of <0.001. These findings were also complemented by a qualitative study that clearly showed the need for information on when to start vaccination and the accessibility of health facilities. A caregiver from Molale 01 kebele with a respondent ID 016 described the need for information as follows: The information that had been provided to me on vaccines was essential, especially when starting the vaccines. I gave birth in a hospital, and the nurse told me to come back on the 45th day. If she did not tell me that was the first visit after birth, then I could not take my child. Many people will lose their vaccination schedule because they do not know when to start their vaccination. Generally, improving the knowledge and awareness of caregivers can help to improve childhood vaccination status. More specifically, as shown by this study, information on when to start vaccination and where to access vaccine significantly affect childhood vaccination status. The findings in this study were also supported by studies conducted in northeast Ethiopia(78) and a systematic review of previous studies conducted in Ethiopia.(79) 9.3 Decision-making and process of getting vaccines related factors and optimum childhood vaccine uptakeDecision-making is one of the most important factors that delay vaccination start date and drop out before completing consecutive doses of childhood vaccines.(80) There are many factors that affect the decision-making process in vaccination. Mainly spouse, immediate family members like father and mother as well as grandfather and mothers play a significant role in influencing the behaviors. Sometimes friends will be important decision-makers in vaccinating children. This study showed that caregivers were the most important decision-makers on vaccination. About 85% of caregivers who participated in this study decided on their own to vaccinate their children. The majority of them got encouragement from their spouse regarding their decision to vaccinate children. This finding agrees with different studies conducted in other countries; a quantitative study(81) and qualitative study(82) findings show the influence of decision-makers like a close family member as essential to complete childhood vaccination. The finding from the qualitative study participants also complements the quantitative study findings. Most of them responded, ‘My husband and I will decide to vaccinate a child.’ This shows that mother and father agree in most scenarios regarding vaccinating a child. Nevertheless, in rare cases, the study showed that the caregiver/mother alone decided to vaccinate a child, and later when the child developed a fever after vaccination, it was found to be a point of disagreement. One caregiver responded about her experience in the following way: “I took my child to vaccination center, and when I came back, she developed fever and crying the whole night, that day my husband was very disappointed, and he said ‘you will never take my child back to vaccination center.’” This shows there are important gaps where fathers should be targeted for a health education program on vaccines. This finding also agrees with a similar study conducted in Ghana.(83) When health facilities are not within a short distance, carrying children and traveling long distances are not encouraging activities to be performed by caregivers. This study showed that about 93% of caregivers travel on foot to get vaccination services. The distance to the nearest health facility ranges from 1km to 18 km, which takes them hours of walking carrying their children. This will discourage caregivers not to starting vaccination as early as possible. On top of this, culturally, it is not acceptable to travel long-distance carrying a newborn child; they prefer to miss their vaccination if health workers are not visiting the caregiver door-to-door for vaccination service. Sometimes, caregivers delay vaccination at 45 days if the child is a female; there is a widely practiced belief saying girls should not be taken out of the home before 80 days, especially among orthodox Christian followers. To sum up, the role of distance from health facilities to residential areas is found to be very important. This study finding was also supported by previous studies conducted in Mozambique(72) and northwestern Ethiopia.(84) The quantitative study was found to be complemented by information collected through qualitative techniques. Caregivers from Kewariat kola kebele stated how this was challenging for them: “…the distance from the health facility is very far, I am not sure, I do not know the exact number of hours we travel, but it will be about eight hours from here. We travel there taking our food because if we arrive in the afternoon, we may not be able to get vaccines and be able to return home the same day. When we returned, my wife felt very tired because she was traveling carrying the child …” After traveling long distances on foot, it is very discouraging for caregivers to see a closed health facility. This study showed that about 31% of the study participants had an experience of returning back before getting vaccines because health facilities were closed or there was an unavailability of vaccines. This finding shows that the problem is worse than the gap identified by the Ministry of Health (MoH). As per the MoH finding, nationwide, only 89.2% of the rural health facilities provide routine immunization services.(6) Sometimes it is not only because there are no vaccines; due to the Ethiopian government’s multi-dose vial policy, there are some vaccines that cannot be opened for a small number of children.(85) Hence, caregivers may be forced to return back without getting the vaccines after waiting long hours in the health facility. The qualitative study showed that this was among areas of complaints by caregivers in the health facility. A caregiver from Molale 01 kebele stated that “… services have been improving and it is good nowadays, but this saying … unable to open the vaccine when children came to the health facility less than 10 is not good. I have seen caregivers leaving the health facility saying I will never come back again in this health facility.” The implementation of a multi-dose vial policy should be careful to be implemented according to the country’s guidelines to avoid the discouragement of caregivers. As caregivers, especially mothers, are responsible for every household activity, this can affect the decision to vaccinate children. Caregivers need to assign someone to the household to replace them in their absence; however, this practice is not easy for caregivers coming from the rural areas of the study areas. The study finding showed that more than 63% of caregivers had difficulty getting someone to delegate household activities when they travel away from home for vaccination services. Findings from the qualitative study also showed similar challenges by caregivers. Almost all of the caregivers had an experience of traveling to the health facilities locking behind their homes and preparing food one day in advance; it is not easy to get even someone who can look after the house from outside. This is not an easy life for rural farmers. Their cattle may travel to ponds and may drink dirty water that has leeches and eventually die when they leave them without someone to take care of. A caregiver from Yigem Kola described their challenges in the following way: It is not easy to get someone who can take care of the house when we travel to health facilities. My wife needs to prepare meals before traveling to a health facility. Regarding the house, we have to lock it, and we say to our neighbors, please look after it. But, no one can be responsible if our cattle went to the river and drank dirty water that had leeches; it usually happens, and they suffer and sometimes die. In a nutshell, vaccination is not an easy activity for farmers; but they must have to choose their children’s health. This study showed that in the decision-making process about full childhood vaccination, the role of spouse encouragement, reminding vaccination date and self-action to recall vaccination schedule, availability of vaccine during health facility visit, and getting someone to delegate household activities were found to be significantly associated with the full vaccination status of children during childhood. (See result section table 11). These are among identified factors that hinder caregivers from visiting a health facility to vaccinate their children. The finding from this study on the availability of vaccines matches with the finding from a previous study conducted in the Gozamin District of the Amhara region to support the findings of this study.(86) Similarly, a study that was conducted to assess the missed opportunity in middle and low-income counties showed similar findings to this study.(87) Some of these challenges can be solved by programmatic changes by the government, while the others still require an effort by caregivers to continue seeking service from a health facility; regardless of their challenges, caregivers should consider the benefits of fully vaccinating their children. Caregivers’ efforts at the individual level also need to be supported strategically through the encouragement of those who successfully completed their vaccination. 9.4 Caregivers’ health facility experience and childhood vaccine uptakeCaregivers’ experience at the health facility is the one that can determine their chance of returning to the same health center for vaccinating children. The finding from this study showed that the majority of them had a good experience in the health facility. However, when we see their interaction with health professionals remains low. As shown by this study, caregivers were not free to interact with health professionals to ask about AEFI and other vaccine-related information. Only 54.3% of them can ask any question about AEFI and other vaccine-related information from their HEWs. This shows the presence of weak points in interpersonal communication skills with HEWs. As this affects the chance of caregivers to return for the next vaccination schedule, programmatic improvements to on interpersonal communication skills of HEWs may be required. A qualitative study conducted in the Benishangul Gumuz region, Ethiopia, agrees with this finding.(88) One way of improving interpersonal communication between caregivers and HEWs is collecting feedback after immunization service. As per the finding from this study, a significant majority of caregivers, 69% of them, were not asked for feedback on the vaccination service before they left the health facility. Feedback is a means where health professionals can learn the challenges of caregivers to access vaccination services. This is missed the opportunity to learn how to improve vaccination service within a health facility and learn about the challenges and experiences of caregivers. The previous study also agrees on the importance of feedback to improve vaccination coverage of consecutive doses.(89) Caregivers usually exchange their feeling among themselves to seek advice from their peers when health professionals are not providing adequate information about the vaccines’ side effects, management of AEFI, benefits of vaccines, and other information. This study showed that about 27% of caregivers heard complaints about the vaccine from other caregivers. If health professionals used this opportunity, most of the caregivers’ concerns and doubt could be solved before they leave the health facility, which would give them the confidence to make a return visit to the same health facility for the next round of vaccination service. This study is supported by previous studies. (90)&(91) Caregivers’ experience of their interaction with a health professional, interpersonal communication, complaints, and other concern was reflected in a qualitative study which can support the finding of a quantitative study. Regardless of the residential area of caregivers, most of them were not asked for feedback after vaccination. Caregivers from Molale town 01 kebele stated her experience of visiting the health facility in the following way: I have seen caregivers waiting in their queue and complaining about the service being provided. I heard them saying, ‘when did this health facility improve its service, and when do we get better treatment?’ It will be good if they organize discussion sessions among caregivers to hear feedback. No one will listen to your feeling, but they tell us when to come next, and they send us home. I had never been asked about feedback. Sometimes they tell you what to do if there is a high fever and swelling at the point of vaccination. Generally, caregivers’ health facility experience plays a very crucial role in the full vaccination status of children. This study also showed that caregivers who experienced closed health facilities, uncomfortable interaction with the health profession, unavailability of vaccines, and hearing complaints from other caregivers within the health facility were found to affect their decision to return to the same health facility for vaccinations services. 9.5 Caregivers’ post-service experience and optimum childhood vaccination
Post-vaccination experience of caregivers includes child discomfort after vaccination, getting a disorganized house, disagreement with spouse due to absence from the house, reaction of the husband, and questions from their community members regarding their experience. This study indicated that nearly half of the caregivers, 48. 2% of those who participated in this study reported that they had experienced vaccine side effects which are limited to fever and swelling at the point of vaccination. After vaccination, health professionals were supposed to explain common side effects and any other Adverse Effect Following Immunization (AEFI) that needs the attention of caregivers. This study showed that 51.5% of caregivers did not receive any health education about vaccine side effects and how to manage it. Consequently, a significant proportion of caregivers, 34.8% of them, were not able to help their children when they faced common side effects, and 52(14%) of caregivers dropped the next vaccination. The finding showed that these factors are significantly associated with childhood full vaccination coverage. This study also supported previous study findings conducted in southern and northwest Ethiopia.(92)&(93) This study collected the feedback of caregivers regarding their overall satisfaction with the service, and most of them rated their experience as good and very good. However, when they were asked whether they could recommend the same service to others, 28.3% of them said they did not like to recommend it. This shows there is an area in the service provider that has to be improved besides other factors which had been discussed related to access, service availability, and interpersonal communication. Caregivers’ satisfaction is one of the important factors that can affect full vaccination status. A previous study conducted in Nigeria and the Southern region of Ethiopia, Hawassa, respectively, agrees with this finding.(94)&(95) As shown by the qualitative study, following a vaccine side effect, there was an occasion when a husband warned his wife not to take the child to the vaccination center. The caregiver explained the situation in the following way: “one day, after the vaccination, I returned home after traveling a long distance. My child was crying all the way from the health facility to home. A few hours after I arrived home, I realized that my child had a high fever. I was very stressed and confused. I did not know what to do. I was giving him breast milk, and he was not sucking. I was very disturbed that day. My husband was also very angry with me. He warned me, saying, ‘you will never take my child to that health facility again.’ Of course, I stopped going to the vaccination center after that day.” This finding also agrees with a study conducted in Nigeria.(94) Another influencer on caregivers will be those community members. Normally, any community member likes to exchange information about health care. Anyone who comes back from a health facility or from the town will be asked to explain what their experience looked like during their visit. The finding from the research supports this. Both the qualitative and quantitative findings showed that the majority of them were asked questions by their community members. From the qualitative study, we learned that most of the questions focused on why they traveled and where they traveled after confirming that they went for vaccination service; they also asked how was their handling was and how the doctor’s behavior. (Sometimes, HEWs are also considered a doctor for the community). This is the way caregivers in the community learn about the services being provided in the health facility before reaching there. If the experience of a caregiver who already visited the health facility was not good, the same experience shared with caregivers who are planning to visit the same health facility would be affected negatively. As the study finding showed, friends’ role in influencing decision-making is also important next to a husband and immediate family member. Hence, someone who had a negative experience with a health facility will not share a positive message. Another challenging experience recorded post-vaccination was related to social responsibilities within their community and the management of their asset, like looking after domestic animals. When caregivers go for vaccination services, they will miss important social gatherings like weddings, funeral ceremonies, and other festivals. These will result in social discrimination. In this study, the result showed that most of the caregivers went to seek vaccination by delegating someone to conduct their social responsibilities on their behalf. However, delegating someone to attend such important events is not easy, or even for those successful to do so, it may not be seen as a full presence by the community members, meaning it still may cause social discrimination. Such kind of discrimination also will influence full child vaccination. On the other hand, as caregivers are leaving their household without anyone to take care of, they may not get a chance to take care of their cows and oxen where they can feed and drink water. The qualitative study revealed that caregivers had experienced that their cattle had drank leeches which caused them suffering and death. The finding from this research showed that household-level activities, including being unable to get someone to delegate for household activities, were found to be highly associated with full childhood vaccination status. however, the researcher was not able to compare these with another study on this particular factor because of limitation of a study conducted in the area. In summary, this research showed that the post-vaccination experience of caregivers is one of bottlenecks for caregivers affecting to vaccinate their children until they complete their childhood vaccines. 9.6 Its implication for policy development and implementationImmunization is one of a strategy the Ethiopian government has been strongly working on to address a significant proportion of community health problems. Vaccination alone will solve childhood sickness and will, reduce the burden on hospitals and reduce unnecessary medical expenditures. In a country like Ethiopia, where many infrastructures like roads and communication are not yet established well, it requires to have a dedicated health policy, program, and structure that can address the need of the community at the grass-root level. From the desk review, we have learned that the country has a policy that gives more attention to the development of a preventive aspect of health care. The health of children was also indicated in the policy as the priority area.(9) The Ethiopian government has been implementing the Health Extension Program (HEP) with an intention to reach rural areas of the community with basic health care like family planning, malaria bed net distribution, vaccination service, and health education activities. However, there are many limitations when it comes to the implementation of the programs like the absence of quality supportive supervision, absence of well-established referral pathway between health post and the next health care level, high turnover of HEWs, absence of career structure for HEWs, unattractive salary and benefits packages inadequate delivery and curative services.(31) These challenges affected the effectiveness of the program, and the findings also showed complementary information like the closure of health facilities during caregiver visits; HEWs did not visit households to check newborn children and encourage vaccinating their children. The result also showed that home delivery is one of the highest in the study area, which compliments one of the shortcomings of the Health Extension Program, the absence of delivery service in the health post. The caregivers’ feedback also showed the constraints of the Health Extension Program, saying, “it could be fine if HEWs visit household for checking newborn children as the caregiver will not visit health facility before the child grow well” culturally, it assumed that it is not fine for the child to take him outside the house before the age of six months to one year assuming that the exposure to sun and wind may cause to him/her sickness. Ethiopia has been implementing the Health Sector Development Programs (HSDP) since 1997, and this health sector program was intended to improve health sector program implementation. The HSDPs is a five-year based program implementation strategy that was initially developed based on the Ethiopian Health Policy; and this has been reviewed every five years, and the next five-year HSDP has been formulated based on gaps seen from the previous HSDP. As the HSDP is based on the country’s health policy, maternal and child health remains the core area of the program, which also tried to address the Millennium Development Goals and now Sustainable Millenium Development Goals (SDG). The HSDP IV indicated that it was intended to achieve a full immunization coverage of 90%.(96) However, eight years later after this program was developed, the Ethiopian Demographic and Health Survey 2018 showed that the full immunization coverage remained at 38.5%. This result indicated that HSDP and the national health policy lack something in terms of improving childhood full vaccination coverage. The Ethiopian Nation Expanded Program on Immunization (ENEPI) has been implemented in Ethiopia for several decades, including the last revised one in April 2015 to be implemented as a multi-year strategy from 2016 to 2020 to address the immunization gaps. The EPI program in Ethiopia was developed to achieve 100% full immunization coverage for children aged less than two years by the year 1990. However, this is not yet successful even after three decades. This program has been implementing different approaches like Reaching Every District (RED) and Sustainable Outreach Service (SOS) to optimize the coverage in remote areas, especially in Afar, Somali, Gambella, and Benishangul regions.(6) However, besides implementing the Health Extension Program in more developed regions like the Amhara region where this study was conducted, despite the presence of some remote areas, there was no clear strategy indicated to address vaccination coverage gaps. On top of the outreach campaigns during an outbreak, the implementation of SOS seems less effectively implemented. Generally, although the presence of a national health policy in Ethiopia since 1997 clearly highlighted the need for emphasis on the preventive aspect of health care, all implementation strategies like the HSDP, national EPI, HEP have been implemented in the country for more than three decades, and the country’s full childhood vaccination coverage remains 38.5%. This shows the presence of a clear gap in policy and strategy planning and implementation. 10) Conclusion and recommendation10.1 ConclusionEven though vaccines have been benefiting global nations in many ways, access to vaccines and utilization remains a challenge in many places. Children living in developing nations are among the disadvantaged in getting access to the vaccine. Ethiopia is one of few countries where millions of children are missing their childhood vaccination. The problem for low vaccination coverage is multi-faceted; it can be linked to access to vaccines, low awareness about vaccines, wrong beliefs about vaccines, and poor service delivery. This study tried to assess factors contributing to low childhood vaccine utilization from the perspective of caregivers. The finding showed that factors that contributed to low childhood full vaccination status were related to the sociodemographic characteristics of caregivers like educational status and residential areas, caregivers’ knowledge about vaccine and vaccination, and pre-and-post health facility experiences. Decision-making to vaccinate a child in this study area requires determination because of several factors like the presence of competing priorities, challenges of getting someone to delegate for the household task, and encouragement to travel to the vaccination site/health post. The finding showed that a caregiver has to weigh the benefits of childhood vaccines over those essential family and social responsibilities before deciding to travel to a health center that requires hours of travel. Inter-personal communication skills of frontline health workers or HEWs play a very significant role in improving service utilization in any health facility. Good communication skills of HEWs can help to improve the service uptake by a caregiver and help to improve their experience in the health facility. This study showed that caregivers who had the best experience in health facilities, including good communication regarding AEFI management and follow-up schedule, people tend to return for a vaccination service. Generally, this study showed that the overall childhood full vaccination coverage was 59%, still one of the lowest and far from the World Health Organization recommendation. In this study, both qualitative and quantitative findings showed that sociodemographic characteristics, knowledge, and awareness of vaccination dates and where to get a vaccination, another decision making, and process-related factors, and pre and post-vaccination experience of the caregivers were found to be factors that had affected childhood full vaccination status. 10.2 RecommendationImproving childhood vaccination coverage requires a coordinated effort, and the challenge can be solved through programmatic improvement and behavior changes. Based on this study’s findings, the following recommendation should be considered for improving the vaccination coverage of the North Shoa Zone.
In general, the regional health bureau and zonal health office should work together with its key partners to improve immunization service accessibility, vaccine promotion, and interpersonal interaction between caregivers and frontline health workers like HEWs and volunteers, including kebele leaders for improved childhood full vaccination coverage. 10.3 Contribution of this studyThe contribution of this study can be seen in terms of its finding and methodology test, the influence of the result on future strategies for immunization, and opening door for future researchers to use the caregiver’s journey to immunization to assess similar challenges of seeking health care for children.
Generally, this study is the first study conducted in the area particularly to assess factors that had been contributing to low childhood vaccination coverage, and it used a new and different approach to study factors from the perspective of caregivers’ experience all the way from household to the health facility and back home, as a researcher this will encourage future public health and behavioral science researchers to study further employing a similar approach.
[1] Ministry of Health, “Heath Policy of the Transitional Government of Ethiopia,” 1993, 11–15. [2] Leif, Gothefors, “The Impact of Vaccine in Low and High Income Countries,” Umea University (October 2, 2008): 55. [3] Anne Geweniger and Kaja M. Abbas, “Childhood Vaccination Coverage and Equity Impact in Ethiopia by Sociodemographic, Geographic, Maternal, and Child Characteristics,” Vaccine 38, no. 20 (April 29, 2020): 3627–3638.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||