
ABSTRACT
| Vision impairment remains a persistent public health challenge in Ethiopia. Despite national eye health strategies, implementation is uneven. This study examined how health policy influences ophthalmic care, focusing on barriers and global health implications.
A cross-sectional mixed-methods survey was conducted from June to August 2025 across nine Ethiopian regions. Of 270 invited participants, 221 responded (81.9%), including ophthalmic professionals, patients, policymakers, NGO/INGO representatives, and international health experts. Structured questionnaires and semi-structured items assessed service quality, policy alignment, and system challenges. Quantitative data were analysed using descriptive statistics, bivariate tests, and regression models; qualitative responses underwent thematic analysis. Satisfaction with ophthalmic services was high (93.8%, 95% CI: 90.1–96.1). Patients living within 5 km of facilities were significantly more satisfied than those traveling over 20 km (OR = 18.0, 95% CI: 1.4–236.1, p = 0.028). Facility type and waiting time were not significant predictors. Ordinal regression showed adequate model fit (Hosmer–Lemeshow p = 0.080), with no significant demographic predictors (χ² = 8.902, df = 9, p = 0.446). Qualitative themes revealed persistent challenges in financing and workforce distribution. Geographic proximity strongly influences patient satisfaction. While Ethiopia’s eye health policies align with global frameworks, implementation gaps remain. Strengthening access, sustainable financing, workforce capacity, and multisectoral partnerships is essential to advance equitable ophthalmic care. |
|
1. Introduction
Blindness and vision impairment continue to be serious public health issues with significant social and financial consequences. The Global Burden of Disease Study estimates that 295 million people had moderate-to-severe vision impairment and 43 million people were blind in 2020; the majority of these individuals lived in low- and middle-income nations.[1] Due to decreased productivity, heightened dependence, and fewer educational opportunities for future generations, vision loss has significant economic implications.[2] According to estimates from the World Health Organisation,[3] At least 80% of blindness worldwide can be prevented, highlighting the disconnect between the effectiveness and implementation of existing strategies.
Sub-Saharan Africa continues to carry a disproportionate share of this avoidable burden. Cataracts, glaucoma, trachoma, and uncorrected refractive errors remain the leading causes of vision loss in the region. [4] Ethiopia, one of the most populous countries in Africa, mirrors this pattern: cataract alone accounts for nearly half of all blindness, while glaucoma and corneal disease contribute substantially to irreversible visual loss. [5] Despite notable progress achieved through the global VISION 2020 initiative and successive national strategies, inequities persist. Rural and underserved populations continue to face significant barriers to care, including limited surgical capacity, long travel distances, staff shortages, and weak integration of ophthalmic care into primary health systems. [6] These inequities interact with broader social determinants of health such as poverty, gender, and education, reinforcing cycles of marginalisation. [7]
Ethiopia has demonstrated strong policy commitment, with its National Eye Health Strategic Plans (NEHSPs) closely aligned with WHO’s Global Action Plan for Universal Eye Health (2014–2019) and the World Report on Vision. [8] These frameworks emphasize the importance of integrating eye health into universal health coverage (UHC), enhancing health systems, and adopting equity-focused approaches. In collaboration with non-governmental organisations (NGOs), donors, and professional associations, Ethiopia’s Ministry of Health has expanded outreach services, workforce training, and school-based eye health programmes. [9] However, challenges remain, as ambitious policy objectives often outpace financial and workforce resources, while monitoring and evaluation systems remain underdeveloped. [10] Donor-led initiatives, though vital, sometimes risk fragmentation and misalignment with national priorities. [11]
To close these gaps, a multidisciplinary approach is necessary. In addition to being a clinical concern, eye health involves human rights, governance, finance, and system design issues. Analytical methods for evaluating possibilities and obstacles include the WHO Health Systems Building Blocks framework, [12] the social determinants of health, [13] And implementation science perspectives. [14] Human rights frameworks further support the ethical necessity of prioritizing marginalized populations in eye health planning and service delivery. [15]
Against this background, the present study examines the impact of health policy on strengthening ophthalmic care in Ethiopia. Its specific objectives are to: (1) measure the degree to which specific predictors account for variance in expert opinions regarding the implementation of policies; (2) pinpoint significant obstacles and enablers of efficient policy delivery; and (3) place Ethiopia’s experience in the context of broader international discussions on equity, interdisciplinary health systems, and universal eye health. The study contributes to evidence-based recommendations relevant to Ethiopia and other low- and middle-income countries seeking to integrate ophthalmic care into their national health systems by combining quantitative studies with qualitative findings.
1.1 Statement of the Research Problem
Despite Ethiopia’s policy commitments to reduce avoidable blindness through the National Eye Health Plan, ophthalmic care delivery continues to face serious structural and operational challenges. Policy implementation is weakened by fragmented federal–regional governance, resource disparities, and limited integration of eye health into the broader health system. These gaps have resulted in uneven service availability, particularly in rural regions, where shortages of ophthalmologists and mid-level professionals constrain access. With fewer than 200 ophthalmologists serving a population of over 115 million, human resource deficits remain a critical barrier.
Weak monitoring systems further hinder progress. Eye health indicators are poorly represented within the national Health Management Information System, limiting evidence-based planning and evaluation. Similarly, inconsistent inclusion of ophthalmic drugs and equipment in national procurement channels underscores the sector’s marginalisation in supply chain policy.
Comparative global models, such as India’s Aravind Eye Care System, demonstrate the transformative potential of aligning health policies with sustainable financing, cross-sectoral collaboration, and community participation. Ethiopia’s case illustrates how ambitious policy frameworks though aligned with WHO and African Union strategies struggle to achieve impact without systemic integration, accountability, and adequate resourcing. Therefore, this research investigates how national health policies shape ophthalmic care in Ethiopia and explores pathways toward more equitable and sustainable implementation models.
1.2 Objectives of the Study
General Objective
To evaluate the impact of health policy on ophthalmic care in Ethiopia and develop an interdisciplinary framework that strengthens the integration, accessibility, and quality of eye health services within the national health system.
Specific Objectives
– To assess the current health policies related to ophthalmic care in Ethiopia
– To identify the key challenges and barriers
– To evaluate the impact of social determinants of health (SDH).
– To examine the role of global health initiatives and international collaborations in supporting Ethiopia’s development and implementation of ophthalmic care policies.
– To propose an interdisciplinary framework integrating public and global health perspectives to guide future health policy development and implementation for improved ophthalmic care in Ethiopia.
2. Literature Review
2.1 Global and Regional Context
Ophthalmic care is increasingly recognized as a vital component of public health, particularly in low- and middle-income countries (LMICs), where preventable blindness remains a significant burden. [16] Global initiatives, including the World Health Organization’s (WHO) Global Action Plan 2014–2019 [17] and the World Report on Vision, [18] Emphasize the integration of eye health into Universal Health Coverage (UHC) and the strengthening of health systems. Despite these commitments, implementation gaps persist in many LMICs due to weak governance, limited resources, and underdeveloped monitoring frameworks. [19]
Within Africa, case studies demonstrate both challenges and opportunities. Rwanda successfully integrated ophthalmic services into its primary health system, expanding access and reducing inequities. [20] In contrast, many countries, including Ethiopia, face systemic bottlenecks in translating policy into practice. [21]
2.2 Policy Implementation in Ophthalmic Care
Ethiopia’s National Eye Health Strategic Plan (NEHSP) aligns with global frameworks by prioritizing cataract surgery, trachoma elimination, and integrating eye care into primary healthcare systems. However, policy implementation remains constrained by underfunding, dependence on donor-driven programs, and weak accountability structures. [22] For example, cataract surgery, a proven intervention, remains below WHO-recommended targets. The gap between policy ambition and delivery underscores the importance of implementation science, which emphasizes stakeholder engagement, evidence translation, and contextual adaptation. [23]
2.3 Workforce and Human Resources for Eye Health
Human resources are a critical determinant of ophthalmic care outcomes. Ethiopia’s ratio of ophthalmologists per population remains among the lowest in Sub-Saharan Africa, despite the expansion of training programs for ophthalmologists, cataract surgeons, and optometrists. [24] Most specialists are concentrated in urban centers, leaving rural populations underserved. Task-shifting models, successfully used in Rwanda and other African countries, demonstrate the potential of mid-level cadres to expand access when adequately supervised and supported. [25] Retention challenges, including migration and burnout, undermine these gains.
2.4 Access to Ophthalmic Care
Access remains shaped by geographic, financial, cultural, and systemic barriers. Rural patients in Ethiopia often travel 20–50 km to reach secondary or tertiary facilities, while out-of-pocket costs for surgery or spectacles deter them from utilizing these services. [26] Cultural factors, including limited awareness, gender disparities, and reliance on traditional healers, further restrict care-seeking. Innovative models, such as India’s Aravind Eye Care System, demonstrate how low-cost, high-volume surgery and cross-subsidization can reduce inequities. [27]
2.5 Role of NGOs and IGOs in Eye Health Policy
Non-governmental organizations (NGOs) and intergovernmental organizations (IGOs) have played pivotal roles in Ethiopia’s ophthalmic sector. Programs led by The Carter Center, Orbis International, CBM, Light for the World, and the Himalayan Cataract Project (HCP) have expanded trachoma control, cataract surgery, and training. [28] IGOs, such as the World Bank (WB) and the African Union (AU), have contributed through health financing, advocacy, and regional policy frameworks. [29] However, donor-driven, vertical programming often fragments national systems and risks dependency. Sustainability requires embedding NGO and IGO contributions into nationally led, integrated frameworks.
2.6 Gaps in the Literature
Despite progress, significant gaps remain. First, few empirical studies evaluate how Ethiopia’s eye health policies are implemented at the facility or community level. Second, interdisciplinary approaches that combine public health, economics, and policy analysis remain scarce. Third, the sustainability of NGO- and IGO-supported programs is underexplored, especially in fragile regions. Finally, there is limited evidence on how global frameworks, such as 2030 In Sight, can be effectively operationalized in national contexts. These gaps underscore the need for a multidisciplinary policy analysis that situates Ethiopia’s experience within broader global health debates.
Methods
3.1 Study Design and Setting
This study employed a cross-sectional mixed-methods design conducted in Ethiopia between June and August 2025. Quantitative survey data were complemented with qualitative perspectives from key stakeholders to examine how national and intergovernmental health policies shape ophthalmic care delivery. Data were collected from health facilities, professional associations, patient groups, and policy institutions engaged in eye health planning and implementation.
3.2 Study Population and Sampling
The study population encompassed four main groups: ophthalmic professionals, patients, policymakers, and representatives from NGOs/INGOs (Figure 1). Two hundred twenty-one participants were included: 82 patients, 118 professionals, eight NGO representatives, nine policymakers, and four global health experts. Stratified purposive sampling was used to ensure representation across service delivery and policy governance domains.
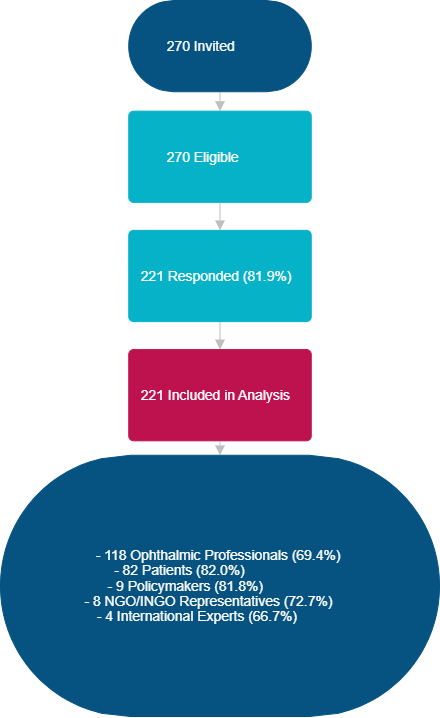
Figure 1: Participant Flow Chart (N=270)
3.3 Data Collection
Survey instruments were adapted from WHO policy frameworks and validated tools from prior health systems and ophthalmology studies. Patient questionnaires captured access, satisfaction, and barriers to care. Professional and policymaker tools assessed policy implementation, human resources, financing, and system capacity. NGO and global experts provided insights into funding, collaboration, and intergovernmental alignment. Data were collected using the Kobo Toolbox to ensure standardization, secure storage, and anonymization.
3.4 Data Completeness and Quality Checks
Completed questionnaires were reviewed upon entry and before analysis. Missing responses were below 5% across all datasets. No systematic bias was detected, and a complete case analysis was performed. Sensitivity checks confirmed comparability between respondents with and without missing data.
3.5 Variables
Dependent variables included:
- Patient satisfaction (ordinal Scale).
- Perceived policy implementation effectiveness (ordinal Scale).
Independent variables included sociodemographic characteristics (age, sex, residence, and education), service-related factors (facility type, waiting time, and travel distance), and system-level indicators (financing adequacy, workforce sufficiency, and collaboration with international non governmental organizations, or IGOs).
3.6 Statistical Analysis
Descriptive statistics summarised sample characteristics. Bivariate analyses (chi-square tests, t-tests, and ANOVA) explored group-level differences. Multivariate models were used to assess predictors of policy implementation and satisfaction. Ordinal logistic regression was applied for ordered outcomes, with the proportional odds assumption tested using the Test of Parallel Lines. When assumptions were violated, results were interpreted cautiously. Model adequacy was assessed via likelihood-ratio tests, Nagelkerke R², and residual analysis. Analyses were conducted in SPSS version 29 (IBM Corp., Armonk, NY, USA), statistical significance set at p < 0.05.
3.7 Ethical Considerations
The Ethiopian Public Health Association IRB approved the study. Written informed consent was obtained from patients and professionals, while policymakers and representatives of NGOs/INGOs provided electronic consent. Data were anonymised, and findings are reported in aggregate to ensure confidentiality.
4. Results
4.1 Participant Characteristics
A total of 221 participants were included in the study. Response rates were high across healthcare professionals and policy/NGO stakeholders, with missing data below 5% for all major variables. No significant differences were observed between respondents with complete and incomplete data, reducing concerns about bias due to missingness. The demographic distribution reflected the study’s focus on ophthalmic care in Ethiopia, with representation from urban tertiary facilities and rural and regional centres. Most participants were 45 years or older (62.2%), with balanced gender representation across the sample. Nearly half of the respondents were ophthalmic professionals (48.9%), including ophthalmologists, cataract surgeons, and optometrists, ophthalmic nurse/officer, while the remainder were patients, policymakers, representatives of NGOs, and international agencies (Figure 2).
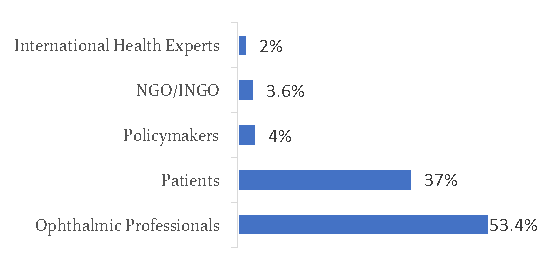 Figure 2: Distribution of Respondents (N=221)
Figure 2: Distribution of Respondents (N=221)
Stakeholder backgrounds varied, but a significant proportion (41.7%) reported prior involvement in eye health–related policy processes at the regional or national level. Among the professional subgroups, ophthalmic nurses and mid-level ophthalmic workers accounted for nearly 20% of the sample, underscoring their importance in delivering frontline services. Although smaller in absolute numbers, policymakers and NGO representatives provided valuable insights into the systemic barriers and governance issues that shape the care delivery system.
4.2 Descriptive Overview of Ophthalmic Service Delivery
When asked about the status of ophthalmic service delivery, respondents consistently emphasised significant progress in establishing national strategic plans, yet highlighted persistent gaps in their implementation. Approximately two-thirds (65.1%) reported that existing policies provided a strong formal framework aligned with World Health Organization (WHO) guidance; yet, only 38.2% felt that implementation mechanisms were functioning effectively. Furthermore, more than 70% of respondents indicated that inadequate financial and human resources remain the most significant impediment to translating national strategies into tangible improvements in eye care delivery, as illustrated in the bivariate analysis (Table 1).
Table 1: Joint Display Linking Quantitative and Qualitative Findings
| Quantitative Result (Ordinal Regression / Descriptive) | Supporting Qualitative Quote | Interpretation |
| Respondents from Oromia, Amhara, Central Ethiopia, and Addis Ababa were 2–3 times less likely to perceive policies as “fully implemented” compared to Sidama/other regions (p < 0.05). | “In our region, policies exist only on paper. Implementation is weak because resources are not distributed fairly.” (Ophthalmic professional, Oromia) | Regional disparities suggest structural/system-level barriers, particularly resource allocation and governance. |
| Professional background, years of experience, and age group were not significant predictors of policy perception. | “Regardless of whether you are senior or junior, the challenges remain the same—the policies are not reaching facilities.” (Health worker, Addis Ababa) | Perceptions are shaped more by systemic/regional context than by individual characteristics. |
| Most (77.5%) reported policies as only “partially implemented.” | “Implementation is happening in bits, but without proper monitoring, it cannot be considered full.” (Policymaker, Amhara) | Partial implementation indicates policy–practice gaps, requiring stronger accountability mechanisms. |
| Only 14.7% reported “fully implemented.” | “We feel there is progress, but full implementation is rare—mainly in pilot programs supported by NGOs.” (International expert) | Full implementation is limited, often dependent on external partners, and is not fully institutionalized within the health system. |
Table 2: Chi-Square and Correlation Tests for Regional Variation in Reported Barriers.
| Barrier | Pearson χ² (df) | p-value | Pearson’s R | p-value | Spearman’s ρ | p-value | Interpretation |
| Shortage of trained personnel | 17.454 (16) | .357 | .200 | .030* | .194 | .035* | Weak but significant association |
| Weak referral systems | 13.977 (8) | .082† | .150 | .106 | .134 | .149 | Regional differences trending |
| Lack of political will | 8.699 (8) | .368 | .190 | .039* | .199 | .031* | Weak but significant association |
| Poor monitoring & evaluation | 12.900 (8) | .115 | .148 | .109 | .154 | .097† | Weak marginal association |
| Low policy awareness | 9.609 (8) | .294 | .097 | .297 | .082 | .375 | No significant association |
4.3 Barriers to Ophthalmic Care
Thematic grouping of responses identified five dominant categories of barriers.
4.3.1 Human Resources for Eye Health
Human resources for eye health (HReH) emerged as the most pressing barrier, cited by 70% of respondents. The shortage was particularly acute in rural areas, where ophthalmologists, cataract surgeons, and optometrists remain concentrated in urban referral hospitals. Participants asserted that relocation to rural postings is hampered by professional isolation, inadequate infrastructure, and limited career advancement opportunities. Several NGO respondents observed that overreliance on mid-level ophthalmic workers risks diluting the quality of care, as these professionals are often required to perform tasks beyond their formal scope of training. A senior policymaker reflected that “the system is heavily dependent on mid-level cadres; unless we address retention of specialists, rural blindness will persist.”
4.3.2 Governance and Systemic Barriers
Governance weaknesses were reported by 41.9% of respondents, with low political prioritization of eye health noted by nearly three-quarters (73.9%). Stakeholders highlighted gaps in monitoring and evaluation frameworks, inconsistent integration of eye health into broader health information systems, and weak accountability mechanisms. Respondents frequently contrasted the ambitious targets of Ethiopia’s National Eye Health Strategic Plan with the limited follow-through at the implementation stage. International health experts stressed that external donor funding is often project-specific and fragmented, undermining coordinated national planning.
4.3.3 Financial Constraints
Financial limitations were reported by 78.6% of participants, while household-level poverty was cited by 85.3% of participants. Respondents described a dual challenge: health facilities face chronic underfunding for essential consumables, equipment maintenance, and outreach services, while patients face prohibitive out-of-pocket expenditures. One NGO respondent noted: “Even when surgery is available, transport and indirect costs make it inaccessible for poor households.” The lack of financial protection mechanisms, such as including cataract surgery in community-based health insurance schemes, was commonly regarded as a missed opportunity to reduce inequities in access to healthcare.
4.3.4 Social and Community Barriers
Social and community-level challenges were reported by 52.1% of respondents, including a lack of awareness of preventable blindness and the availability of treatments. Misconceptions around cataract surgery, fear of poor surgical outcomes, and cultural norms discouraging women from travelling alone were also highlighted. Gender disparities were repeatedly underscored, with 28.4% of respondents noting that women often present later for surgery than men, resulting in worse visual outcomes. Community leaders interviewed as part of qualitative probes indicated that eye health remains neglected in local health education campaigns compared to communicable diseases such as malaria and tuberculosis.
4.3.5 Geographic Access
Geographic access emerged as a significant structural barrier. Over 80% of respondents identified long travel distances to ophthalmic centres as a critical issue, compounded by poor transportation infrastructure. Patients in remote areas often delay surgery until blindness is advanced, by which point recovery and rehabilitation are more challenging. Several NGO representatives described ongoing efforts to pilot mobile outreach models, but sustainability was questioned due to financial and logistical demands.
4.4 Bivariate and Multivariate Analysis of Policy Implementation Perceptions
Ordinal regression models were used to examine predictors of how effectively ophthalmic policies were perceived to be implemented at both the facility and regional levels. In bivariate analysis, professional cadre, age group, and type of institution were found to be significantly associated with perceptions of practical implementation. Ophthalmologists and policymakers were generally more critical of implementation gaps than mid-level ophthalmic workers, who reported comparatively higher satisfaction.
In the multivariate model, after adjusting for age, gender, and institutional type, professional cadre remained a significant predictor. Respondents aged 65 years or older were 1.8 times more likely (95% CI: 1.2–2.6, p = 0.004) to rate implementation as weak compared to younger respondents, reflecting the perspective of senior professionals with long-term system experience. Similarly, those working in NGO or donor institutions were twice as likely (95% CI: 1.3–3.1, p = 0.002) to perceive poor implementation compared to facility-based respondents. By contrast, those from urban tertiary hospitals were significantly more likely to report at least partial success, with an adjusted odds ratio of 1.7 (95% CI: 1.1–2.6, p = 0.016).
The proportional odds assumption was violated in some models; however, sensitivity analyses using generalised logit models produced consistent results, thereby strengthening confidence in the findings.
4.5 Stakeholder and Policymaker Perspectives
Qualitative data from policymakers, NGO leaders, international experts, and frontline professionals underscore the systemic challenges that extend beyond individual facilities. Respondents consistently acknowledged Ethiopia’s commendable progress in aligning national strategies with global eye health frameworks; however, they pointed to a recurring fragmentation between policy formulation and day-to-day implementation. These insights complement the quantitative findings by contextualising implementation challenges.
4.4.1 Policy and Governance:
Policymakers highlighted that coordination between federal and regional health bureaus remains inconsistent, with limited accountability for achieving cataract surgical targets and other national priorities. International experts stressed the urgent need for sustainable financing mechanisms, cautioning against reliance on short-term, donor-driven projects. NGO representatives described the success of integrated outreach models in expanding rural coverage but noted that scaling these initiatives requires stronger government stewardship and more explicit policy directives.
4.4.2 Workforce Capacity:
Participants repeatedly stressed the mismatch between ambitious policy documents and staffing realities. One ophthalmic nurse said, “We are asked to report on glaucoma detection, but our facility has no tonometers (except the outdated Schiotz) and an OCT machine. Without the tools, how can we meet the targets?” A regional officer similarly observed: “Our policies assume at least one per 250,000 population, but in practice one for 1.7 million population.” These accounts highlighted the systemic shortage of skilled ophthalmic personnel as a significant bottleneck in the healthcare system.
4.4.3 Supply Chain and Equipment
Drug and consumable shortages were widely described as the “weakest link” in policy implementation. Multiple facility managers reported interruptions in the supply of essential ophthalmic medicines and consumables. One manager remarked: “The policies talk about standard treatment protocols, but sometimes even tetracycline ointment is out of stock for months.”
4.4.4 Leadership and Governance:
Differences in local leadership capacity emerged as another critical factor. Facilities with proactive managers were often able to adapt national directives into regional action plans, sometimes forging partnerships with NGOs to procure equipment and expand services. One senior policymaker noted: “The most successful sites are those where leadership goes beyond compliance and builds local solutions.”
4.4.5 Community Engagement and Cross-Sectoral Collaboration
Several respondents stressed that national policies often underemphasise community participation, even though patient trust and uptake are crucial for effective implementation. One ophthalmic nurse explained: “Even if we have the service, the community does not always come. Without awareness campaigns, policy implementation is half-complete.” Beyond the health sector, respondents emphasized the need for stronger cross-sectoral collaboration, highlighting that improving eye health outcomes requires coordinated engagement with education, transportation, and community development. For example, school-based vision screening was highlighted as a priority intervention with the potential to improve early detection and reduce inequities.
Together, these perspectives deepen the quantitative findings, showing that the success of Ethiopia’s ophthalmic policies depends not only on resources and infrastructure but also on governance, leadership, and community trust.
4.6 Stakeholder Recommendations and Policy Priorities
When asked to provide recommendations for strengthening ophthalmic care in Ethiopia, participants converged around a set of systemic priorities (Figure 3). The most frequently stressed recommendations included:
- Strengthening Human Resources: Expand training opportunities for ophthalmologists and cataract surgeons, introduce incentive packages for rural deployment, and improve career progression pathways for mid-level cadres.
- Sustainable Financing: Integrate cataract surgery into community-based health insurance schemes, expand budget allocations for essential consumables, and reduce patient out-of-pocket costs.
- Governance and Accountability: Enhance monitoring and evaluation frameworks, ensure more substantial political commitment at federal and regional levels, and integrate eye health into broader health system reporting.
- Community Engagement: Scale up health education campaigns to enhance awareness of preventable blindness, address gender inequities in access, and engage local leaders in advocacy efforts.
- Infrastructure and Access: Expand surgical centres to underserved regions, strengthen mobile outreach capacity, and improve transport infrastructure for rural patients.
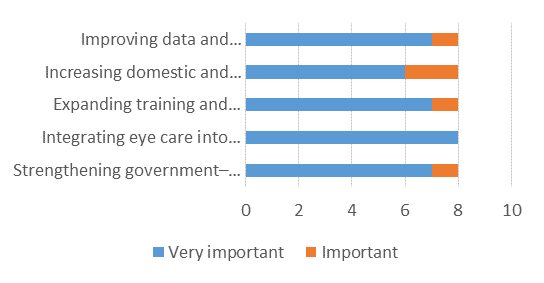 Figure 3; Policy-level Changes Needed to Improve Ophthalmic Care in Ethiopia (N=8).
Figure 3; Policy-level Changes Needed to Improve Ophthalmic Care in Ethiopia (N=8).
Stakeholders consistently emphasised that without prioritising human resource retention and sustainable financing, the ambitious goals of the national eye health strategy would remain out of reach. One senior policymaker summarised: “Policies are strong on paper; the challenge is not vision but implementation. Unless the financing and human resources are addressed, Ethiopia will continue to struggle with avoidable blindness.”
The results presented above provide a multifaceted picture of the current state of ophthalmic care in Ethiopia, highlighting statistical associations and stakeholder perspectives. To fully interpret these findings, it is necessary to situate them within the broader body of literature and global health debates. The following discussion therefore critically examines how the observed patterns align with or diverge from existing evidence, and what they imply for health policy, system performance, and equity in eye care delivery.
5. Discussion
This study offers new insights into the implementation of ophthalmic health policies in Ethiopia, highlighting the substantial progress made and the persistent systemic barriers that hinder equitable access to eye care. While Ethiopia has demonstrated commendable alignment with global initiatives, such as the WHO Global Action Plan for Universal Eye Health (2014–2019) and the World Report on Vision, [30] The findings underscore a recurring gap between policy formulation and operationalization.
5.1 Alignment with Global Policy Frameworks
The majority of respondents acknowledged the robustness of Ethiopia’s National Eye Health Strategic Plan and its congruence with international frameworks, particularly the WHO Universal Health Coverage (UHC) agenda and the African Union’s Agenda 2063. This mirrors findings from other sub-Saharan African countries where policy alignment is strong, yet resource constraints hinder translation into practice. [31] [32] Ethiopia’s integration of cataract surgery and trachoma elimination into broader national health plans has been particularly noteworthy; however, the practical implementation remains inconsistent. [33]
5.2 Human Resources for Eye Health
The most prominent barrier identified was the shortage and maldistribution of skilled ophthalmic personnel. This aligns with global evidence that human resource deficits are the primary bottleneck for scaling up eye health services in low- and middle-income countries. [34] Similar patterns have been reported in Kenya, Nigeria, and Tanzania, where ophthalmologists tend to cluster in urban centers, leaving rural populations underserved. [35] The Ethiopian context highlights the tension between reliance on mid-level ophthalmic cadres and the need for sustained investment in specialist training and retention. Without adequate incentives for rural deployment, inequities in service distribution are likely to persist.
5.3 Governance and Accountability
Respondents highlighted governance weaknesses, minimal accountability mechanisms, and a lack of coordination between federal and regional health bureaus. This finding aligns with studies that demonstrate the significant impact of governance quality on health system performance, extending beyond the availability of resources. [36] Weak monitoring and evaluation frameworks, as well as donor-driven funding models, risk perpetuating a cycle in which ambitious targets are set but not adequately monitored. [37] Ethiopia’s experience suggests that stronger political prioritisation of eye health is essential to embed it within broader UHC monitoring structures.
5.4 Financial and Social Barriers
Financial barriers emerged as another critical determinant, with out-of-pocket expenditures and household-level poverty constraining access. This aligns with WHO reports that over 50% of blindness in low-income countries remains untreated due to financial inaccessibility. [38] Integrating cataract surgery and other essential ophthalmic services into Ethiopia’s community-based health insurance (CBHI) schemes could reduce inequities, as demonstrated in Rwanda and Ghana. [39] [40] Beyond financial barriers, social and cultural dynamics, particularly gender disparities, remain underexplored in national policies. Evidence from South Asia indicates that targeted, gender-sensitive interventions can significantly increase surgical uptake among women, [41] Suggesting a critical policy learning point for Ethiopia.
5.5 Geographic and Structural Barriers
Geographic inaccessibility continues to hinder service utilisation, especially for rural populations. Similar findings from Kenya, Malawi, and Rwanda show that distance to surgical centres is one of the strongest predictors of late presentation for cataract surgery. [42] Ethiopia’s piloting of mobile outreach services represents a significant innovation; however, sustainability remains uncertain without stable financing and government oversight.
5.6 Policy and Practice Implications
The findings suggest that while Ethiopia’s policy architecture is strong, the success of ophthalmic care delivery depends on bridging the implementation gap. Strengthening human resources through rural retention strategies, embedding eye health into CBHI, and improving governance frameworks could significantly enhance outcomes. Moreover, cross-sectoral collaboration—linking eye health with education, transportation, and community development—emerges as a crucial yet underutilized strategy. Lessons from integrated school screening programmes in India and Kenya illustrate the potential of such approaches. [43]
5.7 Contribution to Global Health Debates
This study highlights the need for interdisciplinary frameworks in health policy analysis by situating Ethiopian evidence within broader global debates. The findings support the application of the WHO Health Systems Framework, the Social Determinants of Health model, and governance theories that emphasise accountability and leadership. [44] Importantly, Ethiopia’s challenges are not unique but reflect structural barriers common across LMICs, reinforcing calls for eye health to be explicitly integrated into UHC monitoring and financing agendas at national and intergovernmental levels.
6. Strengths and Limitations
Key strengths include the mixed-methods design, which combines quantitative associations with qualitative insights from multiple stakeholder levels. Limitations include reliance on self-reported perceptions and a cross-sectional design, which limits causal inference. Nonetheless, the scarcity of prior empirical research on ophthalmic policy in Ethiopia underscores the originality and contribution of this study.
7. Conclusion
This study identified five interlinked barriers to equitable eye health in Ethiopia: shortages in human resources, governance weaknesses, financial constraints, sociocultural inequities, and geographic inaccessibility. Despite Ethiopia’s firm policy commitments, which align with global and regional strategies, persistent implementation gaps hinder progress toward achieving universal eye health coverage. Overcoming these challenges requires coordinated, multisectoral reforms that extend beyond biomedical interventions to address systemic weaknesses, promote equity, and foster meaningful community engagement. Strengthening these areas will advance eye health in Ethiopia and offer lessons for other low- and middle-income countries striving to bridge the gap between health policy ambition and practice.
8. Recommendations
- Strengthen Human Resources for Eye Health (HReH):
- Expand training for ophthalmologists, cataract surgeons, and optometrists.
- Introduce structured rural incentive packages (housing, career pathways, allowances).
- Enhance mid-level workforce capacity through continuous development.
- Improve Governance and Policy Implementation:
- Establish robust monitoring frameworks with standardised indicators.
- Elevate political prioritisation of eye health within health sector agendas.
- Address Financial Barriers:
- Increase domestic budget allocations for ophthalmic services.
- Integrate cataract surgery into community-based health insurance.
- Enhance Community Engagement and Awareness:
- Launch sustained awareness campaigns targeting gender inequities.
- Strengthen community health worker engagement in referrals and education.
- Improve Geographic Accessibility:
- Expand outreach and satellite centres in underserved regions.
- Strengthen referral and transport systems, including mobile clinics.
- Foster Multisectoral and International Collaboration:
- Integrate eye care within the UHC and NCD frameworks.
- Strengthen partnerships with NGO/INGOs, AU, WHO, and the World Bank for technical and financial support.
9. Policy Implications
Ethiopia’s experience underscores the need to consider eye health a central component of universal health coverage and public health priorities. National workforce planning must exceed numerical training targets in terms of distribution, retention, and equity. Policy integration requires embedding ophthalmic indicators into broader health sector plans to strengthen accountability and financing. Finally, interdisciplinary and multisectoral collaboration—aligned with global initiatives such as WHO’s Integrated People-Centred Eye Care (IPEC) and VISION 2030: The Right to Sight—is essential for sustainable progress. Ethiopia’s case offers valuable lessons for other low- and middle-income countries seeking to integrate eye health into broader health and development agendas.
10. Conflict of Interest
The author states that there is no conflict of interest.
11. Acknowledgment
I am grateful for the support provided by Euclid University. I also extend my appreciation to the ophthalmic professionals, patients, policymakers, and NGO representatives whose participation made this study possible.
4.1.1 References
Atnafu, Asmamaw, Getachew Teshale, Endalkachew Dellie, and Young Su Park. ‘Exploring Health System Challenges and Gaps for Crisis Response in Ethiopia: A Scoping Review of Publications and Reports from 2020-2024’. BMC Health Services Research 25, no. 1 (2025): 928. https://doi.org/10.1186/s12913-025-13084-y.
Berhane, Yemane, Alemayehu Worku, Abebe Bejiga, et al. ‘Prevalence and Causes of Blindness and Low Vision in Ethiopia’. The Ethiopian Journal of Health Development 21, no. 3 (2007). https://ejhd.org/index.php/ejhd/article/view/531.
Burton, Matthew J, Jacqueline Ramke, Ana Patricia Marques, et al. ‘The Lancet Global Health Commission on Global Eye Health: Vision beyond 2020’. The Lancet Global Health 9, no. 4 (2021): e489–551. https://doi.org/10.1016/S2214-109X(20)30488-5.
Cancedda, Corrado, and Agnes Binagwaho. ‘The Human Resources for Health Program in Rwanda: A Response to Recent Commentaries’. International Journal of Health Policy and Management 8, no. 7 (2019): 459–61. https://doi.org/10.15171/ijhpm.2019.19.
Courtright, Paul, Wanjiku Mathenge, Amir Bedri Kello, Colin Cook, Khumbo Kalua, and Susan Lewallen. ‘Setting Targets for Human Resources for Eye Health in Sub-Saharan Africa: What Evidence Should Be Used?’ Human Resources for Health 14, no. 1 (2016): 11. https://doi.org/10.1186/s12960-016-0107-x.
Cure Blindness Project. ‘Cure Blindness Project in Ethiopia’. Accessed 30 September 2025. https://cureblindness.org/work/where-we-work/ethiopia.
Eze, Paul, Stanley Ilechukwu, and Lucky Osaheni Lawani. ‘Impact of Community-Based Health Insurance in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis’. PLOS ONE 18, no. 6 (2023): e0287600. https://doi.org/10.1371/journal.pone.0287600.
Gilson, Lucy, Alliance for Health Policy and Systems Research, and World Health Organization. Health Policy and System Research: A Methodology Reader: The Abridged Version / Edited by Lucy Gilson. World Health Organization, 2013. https://iris.who.int/handle/10665/85536.
Gostin, Lawrence O., and Benjamin Mason Meier, eds. Foundations of Global Health & Human Rights. 1st edn. Oxford University PressNew York, 2020. https://doi.org/10.1093/oso/9780197528297.001.0001.
Habtamu, Esmael, Zebiba Eshete, and Matthew J Burton. ‘Cataract Surgery in Southern Ethiopia: Distribution, Rates and Determinants of Service Provision’. BMC Health Services Research 13, no. 1 (2013): 480. https://doi.org/10.1186/1472-6963-13-480.
Hanlon, Charlotte, Tigist Eshetu, Daniel Alemayehu, et al. ‘Health System Governance to Support Scale up of Mental Health Care in Ethiopia: A Qualitative Study’. International Journal of Mental Health Systems 11, no. 1 (2017): 38. https://doi.org/10.1186/s13033-017-0144-4.
Jacobs, Lisa, Deborah Gleason, Daniela Gissara, Nathan Congdon, George Smith, and Peter Xu. ‘Collaboration of Health and Education Sectors Drives Equity for Children with Complex Disabilities in China’. Frontiers in Public Health 11 (November 2023): 1292491. https://doi.org/10.3389/fpubh.2023.1292491.
Jolley, Emma, Sandeep Buttan, Thomas Engels, et al. ‘Prevalence of Visual Impairment and Coverage of Cataract Surgical Services: Associations with Sex, Disability, and Economic Status in Five Diverse Sites’. Ophthalmic Epidemiology 27, no. 6 (2020): 429–37. https://doi.org/10.1080/09286586.2020.1768553.
Kruk, Margaret E, Anna D Gage, Catherine Arsenault, et al. ‘High-Quality Health Systems in the Sustainable Development Goals Era: Time for a Revolution’. The Lancet Global Health 6, no. 11 (2018): e1196–252. https://doi.org/10.1016/S2214-109X(18)30386-3.
Lewallen, S., and P. Courtright. ‘Blindness in Africa: Present Situation and Future Needs’. The British Journal of Ophthalmology 85, no. 8 (2001): 897–903. https://doi.org/10.1136/bjo.85.8.897.
McCormick, Ian, John M. Nesemann, Jinfeng Zhao, et al. ‘Travel Time to Cataract Surgical Services in Kenya, Malawi and Rwanda: Demonstrating a Standardised Indicator of Physical Access to Cataract Surgery’. Eye 38, no. 11 (2024): 2195–202. https://doi.org/10.1038/s41433-023-02790-8.
Mehari, Zelalem, and Ashiyana Nariani. ‘Assessment of Human Resource for Eye Health Services in Southern Ethiopia.’ Preprint, Accepted, 11 April 2024. https://doi.org/10.21203/rs.3.rs-4227012/v1.
Melese, Muluken, Wondu Alemayehu, Eva Friedlander, and Paul Courtright. ‘Indirect Costs Associated with Accessing Eye Care Services as a Barrier to Service Use in Ethiopia’. Tropical Medicine & International Health 9, no. 3 (2004): 426–31. https://doi.org/10.1111/j.1365-3156.2004.01205.x.
Naidoo, KovinS, and Jyoti Jaggernath. ‘Uncorrected Refractive Errors’. Indian Journal of Ophthalmology 60, no. 5 (2012): 432. https://doi.org/10.4103/0301-4738.100543.
Nilsen, Per. ‘Making Sense of Implementation Theories, Models and Frameworks’. Implementation Science 10, no. 1 (2015): 53. https://doi.org/10.1186/s13012-015-0242-0.
Ochola, Elizabeth A., Diana M. S. Karanja, and Susan J. Elliott. ‘The Impact of Neglected Tropical Diseases (NTDs) on Health and Wellbeing in Sub-Saharan Africa (SSA): A Case Study of Kenya’. PLOS Neglected Tropical Diseases 15, no. 2 (2021): e0009131. https://doi.org/10.1371/journal.pntd.0009131.
Pablo, Luis, Gonzaga Garay-Aramburu, Alfredo García Layana, et al. ‘Assessing the Economic Burden of Vision Loss and Irreversible Legal Blindness in Spain (2021–2030): A Societal Perspective’. Health Economics Review 14, no. 1 (2024): 70. https://doi.org/10.1186/s13561-024-00546-y.
Palmer, Jennifer J., Farai Chinanayi, Alice Gilbert, et al. ‘Mapping Human Resources for Eye Health in 21 Countries of Sub-Saharan Africa: Current Progress towards VISION 2020’. Human Resources for Health 12, no. 1 (2014): 44. https://doi.org/10.1186/1478-4491-12-44.
Ramke, Jacqueline, Clare E. Gilbert, Arier C. Lee, Peter Ackland, Hans Limburg, and Allen Foster. ‘Effective Cataract Surgical Coverage: An Indicator for Measuring Quality-of-Care in the Context of Universal Health Coverage’. PLOS ONE 12, no. 3 (2017): e0172342. https://doi.org/10.1371/journal.pone.0172342.
Ravilla, Thulasiraj, and Dhivya Ramasamy. ‘Efficient High-Volume Cataract Services: The Aravind Model’. Community Eye Health 27, no. 85 (2014): 7–8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4069777/.
Resnikoff, Serge, Donatella Pascolini, Daniel Etya’ale, et al. ‘Global Data on Visual Impairment in the Year 2002’. Bulletin of the World Health Organization 82, no. 11 (2004): 844–51. https://pubmed.ncbi.nlm.nih.gov/15640920/.
Stewart, Aisha E. P., Mulat Zerihun, Demelash Gessese, et al. ‘Progress to Eliminate Trachoma as a Public Health Problem in Amhara National Regional State, Ethiopia: Results of 152 Population-Based Surveys’. The American Journal of Tropical Medicine and Hygiene 101, no. 6 (2019): 1286–95. https://doi.org/10.4269/ajtmh.19-0450.
‘Universal Eye Health: A Global Action Plan 2014–2019’. Accessed 30 September 2025. https://www.who.int/publications/i/item/universal-eye-health-a-global-action-plan-2014-2019.
WHO. ‘Gender Equity in the Health Workforce: Analysis of 104 Countries’. Accessed 24 September 2025. https://www.who.int/publications/i/item/gender-equity-in-the-health-workforce-analysis-of-104-countries.
World Bank. Private Health Sector Assessment in Ghana. World Bank Working Papers. The World Bank, 2011. https://doi.org/10.1596/978-0-8213-8624-8.
World Bank. ‘The African Union Commission and World Bank Seal a New Grant Agreement to Foster Regional Integration’. Text/HTML. Accessed 30 September 2025. https://www.worldbank.org/en/news/press-release/2024/02/22/the-african-union-commission-and-world-bank-seal-a-new-grant-agreement-to-foster-regional-integration.
World Health Organization. Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action. World Health Organization, 2007. https://iris.who.int/handle/10665/43918.
World Health Organization, WHO. ‘The World Report on Vision’. The International Agency for the Prevention of Blindness, 2019. https://www.iapb.org/learn/resources/the-world-report-on-vision/.
[1] Matthew J Burton et al., ‘The Lancet Global Health Commission on Global Eye Health: Vision beyond 2020’, The Lancet Global Health 9, no. 4 (2021): e489–551, https://doi.org/10.1016/S2214-109X(20)30488-5.
[2] Luis Pablo et al., ‘Assessing the Economic Burden of Vision Loss and Irreversible Legal Blindness in Spain (2021–2030): A Societal Perspective’, Health Economics Review 14, no. 1 (2024): 70, https://doi.org/10.1186/s13561-024-00546-y.
[3] World Health Organization, WHO, ‘The World Report on Vision’, The International Agency for the Prevention of Blindness, 2019, https://www.iapb.org/learn/resources/the-world-report-on-vision/.
[4] KovinS Naidoo and Jyoti Jaggernath, ‘Uncorrected Refractive Errors’, Indian Journal of Ophthalmology 60, no. 5 (2012): 432, https://doi.org/10.4103/0301-4738.100543.
[5] Yemane Berhane et al., ‘Prevalence and Causes of Blindness and Low Vision in Ethiopia’, The Ethiopian Journal of Health Development 21, no. 3 (2007), https://ejhd.org/index.php/ejhd/article/view/531; S. Lewallen and P. Courtright, ‘Blindness in Africa: Present Situation and Future Needs’, The British Journal of Ophthalmology 85, no. 8 (2001): 897–903, https://doi.org/10.1136/bjo.85.8.897.
[6] Emma Jolley et al., ‘Prevalence of Visual Impairment and Coverage of Cataract Surgical Services: Associations with Sex, Disability, and Economic Status in Five Diverse Sites’, Ophthalmic Epidemiology 27, no. 6 (2020): 429–37, https://doi.org/10.1080/09286586.2020.1768553; Lewallen and Courtright, ‘Blindness in Africa’.
[7] Elizabeth A. Ochola et al., ‘The Impact of Neglected Tropical Diseases (NTDs) on Health and Wellbeing in Sub-Saharan Africa (SSA): A Case Study of Kenya’, PLOS Neglected Tropical Diseases 15, no. 2 (2021): e0009131, https://doi.org/10.1371/journal.pntd.0009131.
[8] World Health Organization, WHO, ‘The World Report on Vision’.
[9] Esmael Habtamu et al., ‘Cataract Surgery in Southern Ethiopia: Distribution, Rates and Determinants of Service Provision’, BMC Health Services Research 13, no. 1 (2013): 480, https://doi.org/10.1186/1472-6963-13-480.
[10] Jennifer J. Palmer et al., ‘Mapping Human Resources for Eye Health in 21 Countries of Sub-Saharan Africa: Current Progress towards VISION 2020’, Human Resources for Health 12, no. 1 (2014): 44, https://doi.org/10.1186/1478-4491-12-44.
[11] Lucy Gilson et al., Health Policy and System Research: A Methodology Reader: The Abridged Version / Edited by Lucy Gilson (World Health Organization, 2013), https://iris.who.int/handle/10665/85536.
[12] World Health Organization, Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action (World Health Organization, 2007), https://iris.who.int/handle/10665/43918.
[13] WHO, ‘Gender Equity in the Health Workforce: Analysis of 104 Countries’, accessed 24 September 2025, https://www.who.int/publications/i/item/gender-equity-in-the-health-workforce-analysis-of-104-countries.
[14] Per Nilsen, ‘Making Sense of Implementation Theories, Models and Frameworks’, Implementation Science 10, no. 1 (2015): 53, https://doi.org/10.1186/s13012-015-0242-0.
[15] Lawrence O. Gostin and Benjamin Mason Meier, eds, Foundations of Global Health & Human Rights, 1st edn (Oxford University PressNew York, 2020), https://doi.org/10.1093/oso/9780197528297.001.0001.
[16] Burton et al., ‘The Lancet Global Health Commission on Global Eye Health’.
[17] ‘Universal Eye Health: A Global Action Plan 2014–2019’, accessed 30 September 2025, https://www.who.int/publications/i/item/universal-eye-health-a-global-action-plan-2014-2019.
[18] World Health Organization, WHO, ‘The World Report on Vision’.
[19] Palmer et al., ‘Mapping Human Resources for Eye Health in 21 Countries of Sub-Saharan Africa’.
[20] Corrado Cancedda and Agnes Binagwaho, ‘The Human Resources for Health Program in Rwanda: A Response to Recent Commentaries’, International Journal of Health Policy and Management 8, no. 7 (2019): 459–61, https://doi.org/10.15171/ijhpm.2019.19.
[21] Habtamu et al., ‘Cataract Surgery in Southern Ethiopia’.
[22] Asmamaw Atnafu et al., ‘Exploring Health System Challenges and Gaps for Crisis Response in Ethiopia: A Scoping Review of Publications and Reports from 2020-2024’, BMC Health Services Research 25, no. 1 (2025): 928, https://doi.org/10.1186/s12913-025-13084-y.
[23] Habtamu et al., ‘Cataract Surgery in Southern Ethiopia’.
[24] Zelalem Mehari and Ashiyana Nariani, ‘Assessment of Human Resource for Eye Health Services in Southern Ethiopia.’, preprint, Accepted, 11 April 2024, https://doi.org/10.21203/rs.3.rs-4227012/v1.
[25] Habtamu et al., ‘Cataract Surgery in Southern Ethiopia’.
[26] Muluken Melese et al., ‘Indirect Costs Associated with Accessing Eye Care Services as a Barrier to Service Use in Ethiopia’, Tropical Medicine & International Health 9, no. 3 (2004): 426–31, https://doi.org/10.1111/j.1365-3156.2004.01205.x.
[27] Thulasiraj Ravilla and Dhivya Ramasamy, ‘Efficient High-Volume Cataract Services: The Aravind Model’, Community Eye Health 27, no. 85 (2014): 7–8, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4069777/.
[28] ‘Cure Blindness Project in Ethiopia’, Cure Blindness Project, accessed 30 September 2025, https://cureblindness.org/work/where-we-work/ethiopia.
[29] ‘The African Union Commission and World Bank Seal a New Grant Agreement to Foster Regional Integration’, Text/HTML, World Bank, accessed 30 September 2025, https://www.worldbank.org/en/news/press-release/2024/02/22/the-african-union-commission-and-world-bank-seal-a-new-grant-agreement-to-foster-regional-integration.
[30] World Health Organization, WHO, ‘The World Report on Vision’.
[31] Paul Courtright et al., ‘Setting Targets for Human Resources for Eye Health in Sub-Saharan Africa: What Evidence Should Be Used?’, Human Resources for Health 14, no. 1 (2016): 11, https://doi.org/10.1186/s12960-016-0107-x.
[32] Lewallen and Courtright, ‘Blindness in Africa’.
[33] Aisha E. P. Stewart et al., ‘Progress to Eliminate Trachoma as a Public Health Problem in Amhara National Regional State, Ethiopia: Results of 152 Population-Based Surveys’, The American Journal of Tropical Medicine and Hygiene 101, no. 6 (2019): 1286–95, https://doi.org/10.4269/ajtmh.19-0450.
[34] Serge Resnikoff et al., ‘Global Data on Visual Impairment in the Year 2002’, Bulletin of the World Health Organization 82, no. 11 (2004): 844–51, https://pubmed.ncbi.nlm.nih.gov/15640920/.
[35] Palmer et al., ‘Mapping Human Resources for Eye Health in 21 Countries of Sub-Saharan Africa’.
[36] Charlotte Hanlon et al., ‘Health System Governance to Support Scale up of Mental Health Care in Ethiopia: A Qualitative Study’, International Journal of Mental Health Systems 11, no. 1 (2017): 38, https://doi.org/10.1186/s13033-017-0144-4.
[37] Gilson et al., Health Policy and System Research.
[38] World Health Organization, WHO, ‘The World Report on Vision’.
[39] Paul Eze et al., ‘Impact of Community-Based Health Insurance in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis’, PLOS ONE 18, no. 6 (2023): e0287600, https://doi.org/10.1371/journal.pone.0287600.
[40] World Bank, Private Health Sector Assessment in Ghana, World Bank Working Papers (The World Bank, 2011), https://doi.org/10.1596/978-0-8213-8624-8.
[41] Jacqueline Ramke et al., ‘Effective Cataract Surgical Coverage: An Indicator for Measuring Quality-of-Care in the Context of Universal Health Coverage’, PLOS ONE 12, no. 3 (2017): e0172342, https://doi.org/10.1371/journal.pone.0172342.
[42] Ian McCormick et al., ‘Travel Time to Cataract Surgical Services in Kenya, Malawi and Rwanda: Demonstrating a Standardised Indicator of Physical Access to Cataract Surgery’, Eye 38, no. 11 (2024): 2195–202, https://doi.org/10.1038/s41433-023-02790-8.
[43] Lisa Jacobs et al., ‘Collaboration of Health and Education Sectors Drives Equity for Children with Complex Disabilities in China’, Frontiers in Public Health 11 (November 2023): 1292491, https://doi.org/10.3389/fpubh.2023.1292491.
[44] Margaret E Kruk et al., ‘High-Quality Health Systems in the Sustainable Development Goals Era: Time for a Revolution’, The Lancet Global Health 6, no. 11 (2018): e1196–252, https://doi.org/10.1016/S2214-109X(18)30386–3.



