

ABSTRACT
| Uganda, hosting nearly 1.7 million refugees, began integrating refugees into its National Health System in 2017 to improve access, equity, and sustainability under successive Health Sector Integrated Refugee Response Plans. The study examines the extent of integration using a convergent parallel mixed-methods design.
Quantitative data were collected from 242 refugee patients and caregivers across 22 government health facilities in northern Uganda, complemented by interviews with facility managers and a district health officer. Quantitative analysis used descriptive statistics and regression modelling in STATA, while qualitative data were thematically analyzed. Findings show substantial integration, with 92% of respondents accessing services through government facilities. Overall satisfaction was moderate (85%) and significantly associated with household income (p = 0.047). Strong social cohesion was reflected in high perceived safety within facilities. Access was high for maternal and child health, preventive, chronic, and emergency services, but limited for mental health and disability care. Key challenges included medicine stockouts, staffing shortages, infrastructure gaps, underfunding, language barriers, and limited refugee participation in care delivery. Despite progress, structural and operational constraints persist. The study highlights the need for stronger policy dissemination, health system strengthening, livelihood support, and continued research to achieve equitable and sustainable refugee health integration in Uganda. |
|
- Introduction
Globally, refugees constitute one of the most vulnerable populations, facing acute medical and psychosocial challenges that begin before displacement and often persist long after they find refuge[1]. Several studies have documented forced migration as disruptive to the social support systems, livelihoods, and access to health care, leaving refugees exposed to heightened risks of infectious diseases, malnutrition, and mental health distress[2].
Member states are mandated to provide international support to refugee situations within their borders, but although this interventionist model has historically offered lifesaving relief, it is predominantly short-term, emergency-oriented, and frequently operates through parallel service delivery structures rather than through national systems. Consequently, such arrangements, while expedient during crises, often lead to inefficiencies, fragmented service provision, and a weakened national health system[3].
Uganda presents a particularly relevant experience in refugee protection, pursuing a progressive and inclusive refugee policy anchored in the Comprehensive Refugee Response Framework (CRRF), the 2006 Refugee Act, and the 2012 Refugee Regulations. Despite this conducive and progressive legal framework, there is a paucity of information regarding Uganda’s progress in integrating refugees into the national health system.
1.1. Objectives of the Study
Refugees in Uganda, in principle, have access to the national healthcare system, yet many refugees still complain of limited access to healthcare services. Currently, limited information is available on the extent of refugees’ integration into the Ugandan National Health System. The overall objective of this study is to assess the current status of refugees’ integration into Uganda’s national health system and to identify the extent, enablers, and barriers to integration.
1.2. Specific Objectives
The specific objectives for this study are as follows:
- To assess the extent to which Uganda’s progressive legal and policy framework for refugees’ integration has been operationalized within the national health system, particularly in refugee-hosting districts.
- To identify and analyze the key barriers and enablers influencing the integration of refugee-health services into the national health system.
1.3. Significance of the Study
This study provides an updated status of the integration of refugees into Uganda’s national health system, shedding more light on the barriers and enablers of this integration process. This allows for urgent corrective actions to address the barriers and further strengthen the drivers.
2. Literature Review
2.1. Uganda’s Location and Refugee Population
Uganda is a small country in East Africa, with a land area of 241,038 square kilometers, of which 41,743 square kilometers is water. The country currently hosts over 1.7 million refugees, primarily from South Sudan, the Democratic Republic of the Congo (DRC), Burundi, and Rwanda.[4] Most of these refugees are hosted in the countryside, where access to services is already limited. The map below shows the location of major refugee settlements in Uganda.
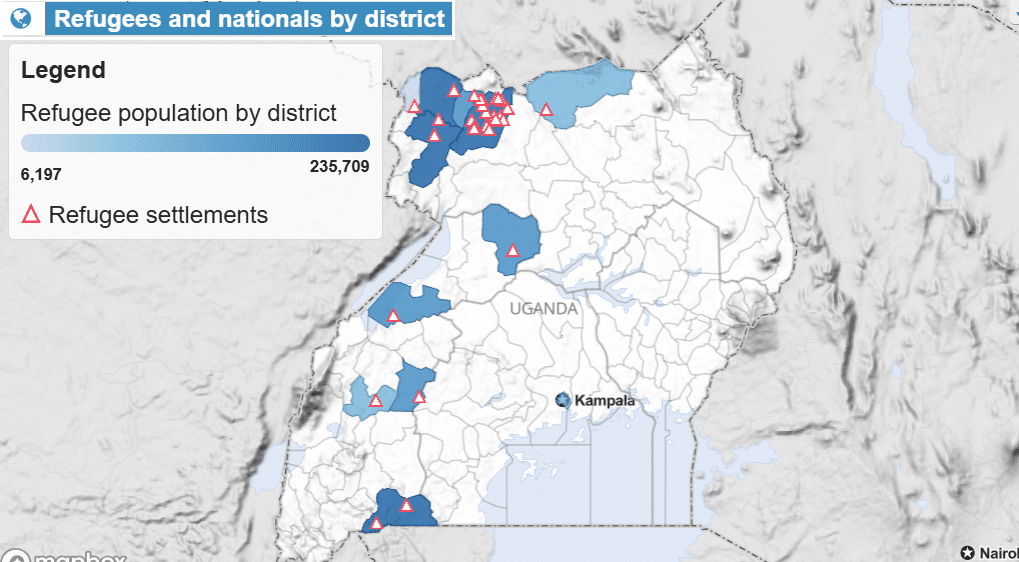
Figure 1: Map of Uganda Showing Refugee Settlements
Adapted from UNHCR Uganda Population Statistics Dashboard – 30 Sep 2024,
2.2. Uganda’s Population Profile and Health System Structure
Uganda’s population of 45.9 million has an annual growth rate of 2.9%, with women and girls comprising approximately 50.7% of the population.[5] This high population growth rate, compounded by continued refugee influx, puts immense pressure on the limited resources available to the national health system. Uganda’s health system operates under a mixed model (Public and private).[6] The public sector provides approximately 75% of total health services, while the private sector (including not-for-profit and for-profit entities) contributes 20%. Health Insurance, primarily for employed workers, covers 5 %.
Uganda’s health service delivery is guided by the National Minimum Health Care Package (NMHCP), which prioritizes essential services but has a limited scope.
2.3. The Economic Status of Uganda
Nearly 42.2 % of Ugandans live below the international poverty line.[7] The age dependency rate in Uganda is high (85.7 per 100 population), meaning that for every 100 working people, there are 86 dependents aged under 18 or over 64.[8] This high age dependency (85.7%) and a low employment-to-population ratio (43%) limit households’ ability to afford private health services.[9] Consequently, refugees who need employment may not easily access job opportunities, forcing both refugees and host communities to rely heavily on public health facilities, further burdening an already resource-constrained system.
2.4. Government Contribution to Healthcare Financing in Uganda
In 2019, private expenditure accounted for 41.4% of Uganda’s current health expenditure, with 95% of this amount being out-of-pocket payments incurred by Ugandans as they sought healthcare. In the same year (2019), the government of Uganda provided 17.2% of the country’s current health expenditure, while donors contributed 41.4%, of which only 21% was in the form of budget support.[10] Current health expenditure (CHE) refers to the amount of money a country spends on healthcare services and goods. Figure 2 below shows Uganda’s health financing streams.
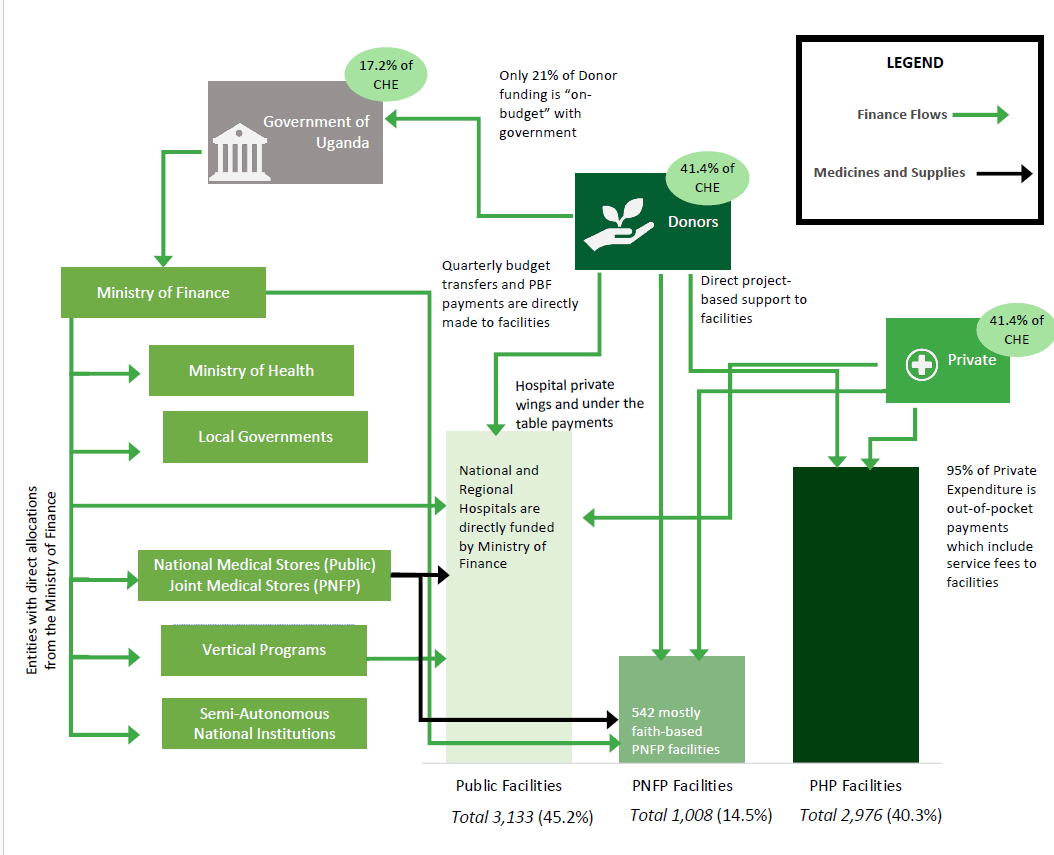
Figure 2: Health Financing in Uganda.
Adapted from Uganda Health Purchasing Factsheet
In 2020/2021, the Ugandan government’s expenditure on health accounted for only 17 % of current health spending, while donors covered half of the funding gap, with the remainder funded by citizens through out-of-pocket health expenditures.[11] High out-of-pocket expenditure reflects inequitable and limited access for the poor and the most vulnerable in the country, such as refugees. Further, in 2018/2019, health accounted for only 7% of the national budget, far below the 15% target set by the Abuja Declaration.[12]
The overall per capita health expenditure in Uganda, including donor contributions, remains at USD 54.[13] This is far below the USD 86 benchmark required to provide essential services in Low- and Middle-Income Countries (LMICs). Additionally, Health insurance accounts for only two to five % of Uganda’s health financing landscape.[14] This illustrates the system’s dependency on external aid, underscoring the fragile state of the Uganda National Health System and the funding gaps for integrating refugee healthcare. Comparative experiences from Kenya and Rwanda, where national health insurance frameworks have progressively incorporated refugees, suggest that a functional National Health Insurance System (NHIS) could significantly improve equity and service continuity.[15]
Weak financial management in the Uganda public service has compounded funding constraints. Audits by Uganda’s Public Accounts Committee revealed systemic inefficiencies and bureaucratic delays that cause under-absorption of healthcare funds. Hospitals such as Lira, Mubende, and Mulago had returned unspent wage funds due to recruitment delays exceeding five months.[16] Such inefficiencies mirror trends in other LMICs, such as Ethiopia and Tanzania, where decentralization has not been matched by adequate local financial management capacity, resulting in similar bottlenecks in human resource deployment, financial management, and procurement.
2.5. Medicines Availability and Medical Supplies
In 2020/21, the availability of tracer commodities in Ugandan health facilities declined from 83 % in 2019/20 to 81 %, falling short of the national target of 90 % stock availability.[17] Stockouts result in nearly one in five patients missing essential medicines or laboratory tests in Uganda. A 2022 cross-sectional survey of 128 health facilities in Uganda found that 84% had experienced stockouts within the previous six months. The major causes of stockouts, as identified by the Budget Monitoring and Accountability Unit of the Ministry of Finance in Uganda, were funding gaps, delivery delays, supply-demand mismatches, and poor record-keeping /logistics management.[18]
These challenges resonate with findings in Kenya and Bangladesh, where limited automation for records management and delivery challenges, including unfulfilled last-mile delivery obligations, undermine drug availability in public facilities.[19] In Uganda, the UNHCR provides additional medicines to refugee-serving health facilities, which are often insufficient to serve refugees and host populations effectively.
2.6. Human Resources for Health
The current health workforce in Uganda is 78 % of the required staffing levels, with a health worker density of 1.6, far below the 4.45 required for Universal Health Coverage.[20] Critical staff shortages persist in referral hospitals and lower-level facilities, where the new staffing structure (introduced in 2019) remains unfunded.
Health staff absenteeism in Uganda, estimated at 69 %, is linked to low pay, delayed salaries, weak supervision, and competing social obligations. Similar patterns of staff absenteeism have been observed across LMICs. In Nigeria and Nepal, absenteeism is correlated with underpayment, poor facility conditions, and a lack of motivation. In Uganda, the office responsible for supportive supervision, the District Health Officer (DHO) position, remains severely understaffed, as only 61 % of DHO positions are currently filled. This limits local oversight and coordination in regions hosting refugees.[21]
2.7. Drivers and Inhibitors of Integration
Integration is undermined by systemic weaknesses, including poor coordination, inadequate infrastructure, stockouts, and human resource gaps, as identified in studies from Adjumani and Obongi.[22] Although the study by Komakech et al. highlights some of the barriers, it falls short of assessing the extent to which the current integration of refugee healthcare into the national health system has been achieved.
2.8. Conceptual Review
The conceptual framework for this study was developed by combining the 2008 conceptual framework for refugee integration by Ager and Strang and the UNESCO conceptual framework for integrating refugees into national education systems. The WHO health system building blocks further supplemented the two frameworks, enhancing clarity.
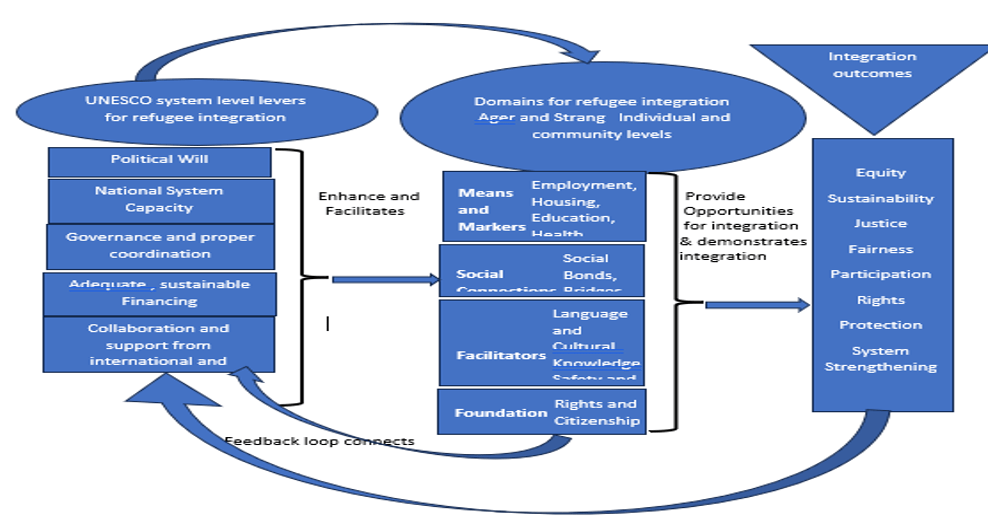
Figure 1: Conceptual Framework for the Study
Researcher‘s own construction
Ager and Strang’s Conceptual Framework for Refugee Integration
Ager and Strang (2008) conceptualize integration across four interrelated domains: Markers and Means, Social Connections, Facilitators, and Foundations. Health is treated as the primary marker of integration, reflecting refugees’ access to, utilization of, and satisfaction with services within Uganda’s national health system. Social connections—through bonds, bridges, and links—inform analysis of equity, inclusion, and relationships between refugees, host communities, and state institutions. Facilitators such as language proficiency and perceived safety shape refugees’ ability to navigate health services effectively. Foundations, grounded in legal status and rights under Uganda’s Refugees Act (2006), determine access to services and influence the sustainability and cost-effectiveness of integrated refugee healthcare delivery[23].
UNESCO’s System Level Levers Framework for Refugee Integration
UNESCO’s system-level levers provide further insight into the key nodes that are crucial for ensuring successful refugee integration into national systems. It thus complements the above conceptual framework, providing greater depth to aid a more comprehensive understanding of the dynamics of refugee integration.
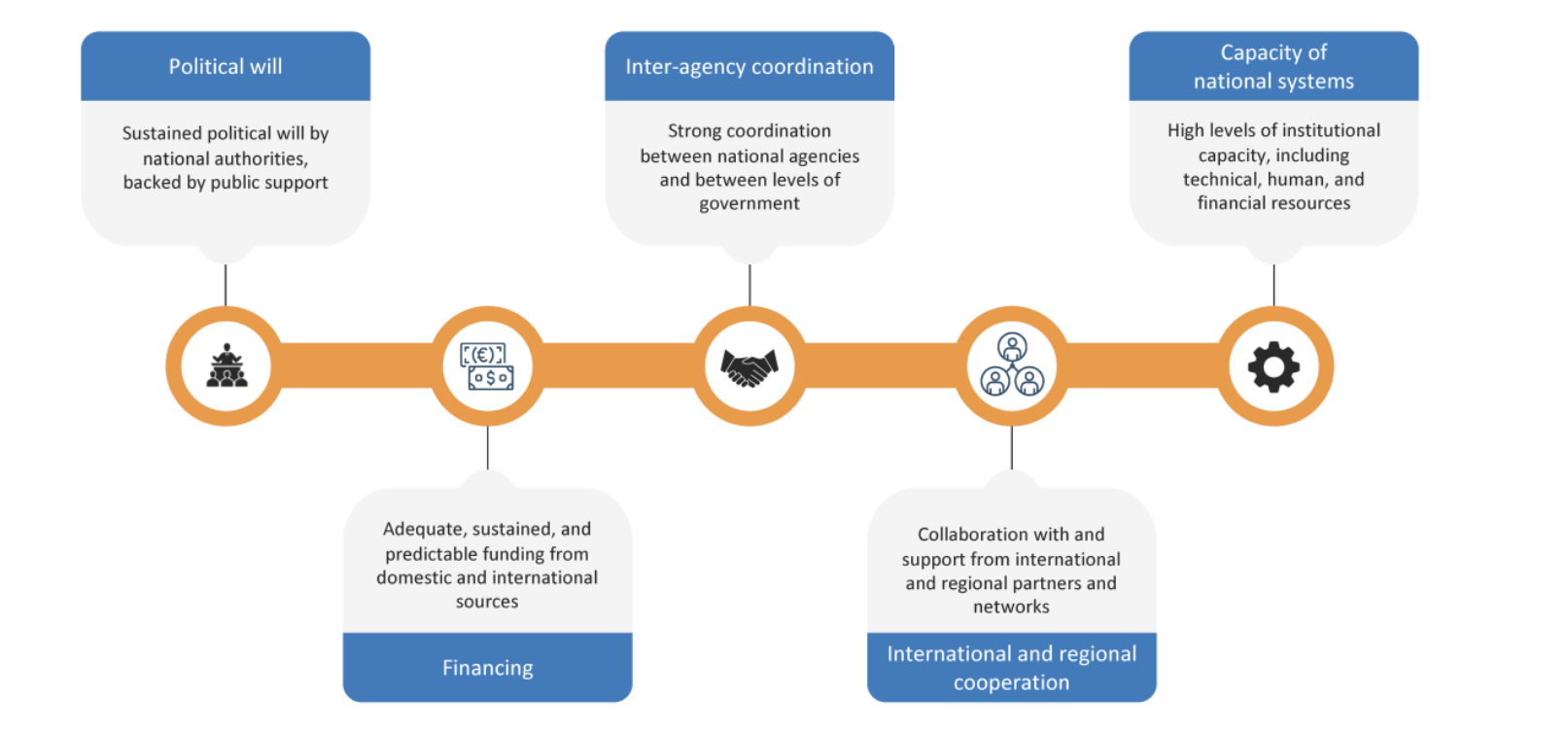
Figure 2: UNESCO’s Conceptual Framework: System-Level Levers for Refugee Inclusion
Adapted from the inclusion of refugees into the national education System, UNESCO.[24]
These five-level system levers depict key nodes in the refugee integration process, enriching understanding of refugee integration within the national system.[25]
2.9. Gaps in the Literature
Prior studies have mostly focused on perceptions or policy analysis, with limited systems-level assessment and minimal inclusion of refugees lived experiences. Several are under-theorized, relying on descriptive or single-framework approaches that fail to account for the gaps between policy and practice. Additionally, governance, accountability, and donor coordination are poorly analyzed, despite evidence of underutilized funding and leadership bottlenecks. This study addresses these gaps through a mixed-methods, system-oriented, and theory-informed approach.
- Methods / Methodology
3.1. Study Design
The study used a convergent parallel mixed-methods design, collected qualitative data from 242 refugee respondents and conducted key informant interviews with nine health facility in-charges and one district health officer. The collected quantitative and qualitative data were analyzed separately, and the findings were compared and corroborated. The mixed-methods approach employed a robust design, enabling synergy between qualitative and quantitative methods, which is necessary for evaluating a complex phenomenon such as refugee healthcare integration. Figure 5 below illustrates the research design.
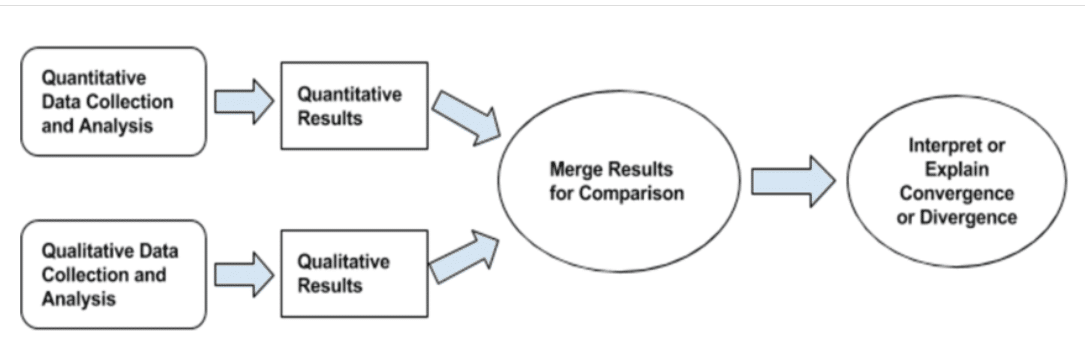
Researcher’s construction
3.2. Study Setting/Area of the Study
This study was conducted in the refugee settlements of Adjumani, Palorinya, and Lamwo, which host nearly 800,000 refugees, including both old and new caseloads. Data were collected from primary and secondary sources. Primary data included key informant interviews and semi-structured questionnaires with refugees, health managers, one referral hospital administrator, and a district health officer. Secondary data were obtained from electronic and published sources, including books, journals, reports, institutional records, and other published and unpublished materials. The Ethical Review Board of Euclid University and the Office of the Prime Minister of Uganda, represented by the Refugee Desk Officer, granted approval for this study. A copy of this study protocol was also shared with the UNHCR Uganda technical team, and the principal investigator received no concerns or queries.
3.3. Inclusion and Exclusion Criteria
For the quantitative arm of the study, each respondent was a refugee patient or caregiver who had visited the health facilities on the day of the interview to seek healthcare services for themselves or a family member. A refugee caretaker was taken as a respondent only if her patient was unable to engage or was a minor. Only eligible refugees who provided written informed consent were included in the study.
3.4. Sampling Frame for Quantitative and Qualitative Interviews
The sample size calculation for the quantitative arm of this study was based on Cochran’s formula, which provides the most accurate estimate for proportions when the study population is infinite. Based on anecdotal information, the proportion of refugee integration into the Uganda National Health System was estimated at 80%. The confidence level was 95%, yielding a total sample size of 246 respondents. All 26 health facilities in the study area constituted the sampling frame, from which 21 were randomly selected for the quantitative study. Each health facility provided 12-15 respondents obtained through systematic sampling, selecting every seventh refugee patient from the outpatient register on the interview date. This systematic sampling reduced the likelihood of response clustering. The total number of valid responses analyzed was 242, yielding a response rate of 98.4%. For qualitative data, nine facilities were randomly selected, and one referral hospital was purposively included. Nine health facility managers and one district health officer were interviewed.
3.5. Validity and Reliability Strategies for Qualitative and Quantitative Tools
Ten trained health worker research assistants, fluent in refugee languages and experienced with Kobo Collect, conducted data collection, leveraging existing trust to encourage open responses. A pretest with 27 respondents (11% of the sample) identified and corrected gaps in the tools. Health facility checklists verified staffing, medicine stocks, financing, supply chains, and governance ststus. Data quality and confidentiality were ensured through informed consent, anonymity, unique identifiers, and Kobo self-validation rules enforcing completeness and skip patterns. Daily data synchronization and review by the principal investigator and supervisors identified and corrected errors. Duplicate, incomplete, and inconsistent entries were removed during data cleaning.
For secondary data, a systematic search across PubMed, Scopus, Web of Science, and Google Scholar, complemented by grey literature sources (including reports from UNHCR, WHO, and the Government of Uganda), yielded 742 records. After removing 126 duplicates and those with irrelevant geographical focus, 616 records remained for title and abstract screening, of which 412 were excluded as irrelevant to refugee health or lacking a focus on integration into the host country’s health systems. Of the remaining 204 full-text articles and reports assessed for eligibility, 88 were excluded because they were either outdated, lacked empirical data on integration, were incomplete, or lacked methodological rigor. Finally, 116 studies met the inclusion criteria and were retained for detailed review and synthesis. Of these, 66 were peer-reviewed journal articles, while 50 were policy documents and other types of grey literature.
Qualitative interviews were conducted with nine health managers, including eight from settlement health facilities, one district hospital administrator, and a district health officer. This explored the health system’s capacity, gaps, and challenges affecting the integration of refugee health. While health facilities were randomly selected, managers were purposively sampled; and snowball sampling was used to identify the next suitable respondent in health facilities where the managers were unavailable. Semi-structured interviews examined governance, financing, service delivery, coordination, and sustainability. Interviews were audio-recorded, transcribed verbatim, and complemented by facility checklists on human resources, medicines, and governance. Data were analyzed thematically using Braun and Clarke’s framework, with open coding, theme development, and iterative refinement. Findings were triangulated with quantitative data, literature, and health system records.
- Results
Demographic Characteristics of Respondents
Table 1: Characteristics of Study Respondents
| Characteristic
|
N = 2421 |
| Age | 30 (24, 38) |
| Sex | |
| Female | 171 (71%) |
| Male | 71 (29%) |
| Education Level | |
| A- level | 7 (2.9%) |
| None | 40 (17%) |
| Primary | 128 (53%) |
| Secondary | 67 (28%) |
| Employment status | |
| Business/shop/market stall owner | 5 (2.1%) |
| Formally Employed | 4 (1.7%) |
| Others | 20 (8.3%) |
| Peasant | 69 (29%) |
| Retired | 1 (0.4%) |
| Self Employed | 15 (6.2%) |
| Un employed | 128 (53%) |
| Years of stay in Uganda | |
| 5 to 8 years | 116 (48%) |
| Less than 5 years | 6 (2.5%) |
| More than 8 years | 120 0%) |
4.1 Knowledge of Policies Regarding Refugee Access to Healthcare
This study confirmed the presence of policy and legal documents including the Uganda Refugee ACT 2006, the Constitution of the Republic of Uganda, and the Refugee Regulations of 2010, which collectively grant refugees the right to access national services on the same basis as other non-citizens. These policy documents and successive National Development Plans provide a basis for the much recognized progressive refugee protection regime in Uganda. The Refugee Act 2006 CAP 29 (d) specifically allows refugees equal treatment as any other foreigner in Uganda[26]. The 2010 Refugee Regulations specifically recommend integrating refugee issues into national and district development planning. In addition, the Health Sector Integrated Refugee Response Plan 2019–2024 requires district local governments to include refugees in health planning, monitoring, and service delivery. However, despite this enabling framework, the study found a significant implementation gap, with approximately 50% of health facility in-charges in settlement areas unaware of existing refugee health policies, potentially limiting effective and consistent service provision.
4.2 Physical and Functional Access to Health Services
The study found adequate health facility distribution in the study area, with 93% of respondents walking less than 90 minutes to reach care. Health facilities were closely spaced, with overlapping 5-kilometer catchment areas. However, functional access was limited by critical health system gaps, including medicine stockouts, staff absenteeism, and governance challenges. Furthermore, 41 (17%) respondents reported a limitation in the scope of health services as a critical barrier to healthcare access in the settlement.
4.3 Health Service Satisfaction and Sense of Comfort
Most respondents (218, 90%) felt welcome and comfortable accessing health services at nearby government health facilities. Up to 239 (99%) respondents reported that they were more likely to recommend the health facilities to their family members and friends for care. However, overall satisfaction with health services was moderate, 206 (85%).
4.4 Health Services Accessed by Refugees
The most accessed health services were as follows: Maternal and Child Health (58%), Preventive Health (52%), Emergency care (47%), and Chronic Disease Care (34%). Significant unmet needs persisted in mental healthcare and disability-related services, including vision care. Mental health services were especially underprioritized despite refugees’ trauma exposure, as one health center III serving about 27,000 people had only one trained clinical mental health staff.
4.5 Social Integration and Refugee Participation in Governance and Development
This study highlights the importance of safety and social integration in facilitating refugees’ access to healthcare. Findings show strong social bonds and bridges with host communities: 10% shared the same language, 62% attended the same churches, 94% used the same markets, 42% participated in the same social functions, 16% joined the same savings groups, and 64% reported their children played together. Most respondents had good neighborly relations (224, 92.57%) and felt safe in government health facilities (240, 99%).
However, social links in governance were weak: only 53 (22%) were often consulted in planning, 72 (30%) were never consulted, and 116 (47%) were occasionally consulted.
4.6 Barriers to Healthcare Access Among the Refugees
Figure 7 below presents the major barriers to refugee health care access in this study.
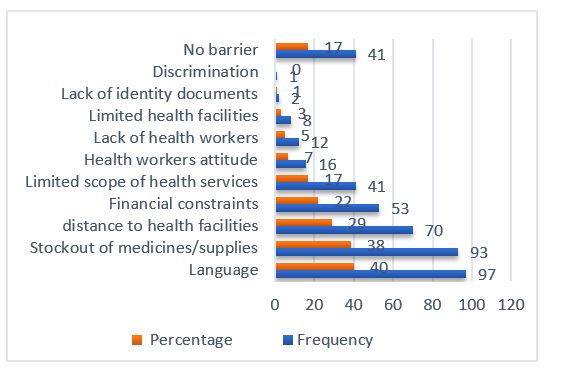
Figure 7: Key Barriers to Healthcare Access Among Refugees
Language and Communication Challenges
Language was the most mentioned barrier to healthcare access in this study. A total of 97 respondents (40%) reported language as a barrier to accessing healthcare. Language was a bigger barrier for women than men, as 71(73.1%) of those who reported language as a barrier to health access were women. Language and communication barriers were more of a problem in Palorinya Refugee settlement, followed by Adjumani and Lamwo Settlements.
Stockout of Medicines and Medical Supplies In the Settlement Health Facilities
Stock out of essential medicines was reported by 92 respondents (38%) as a key barrier, and 96 (40%) of dissatisfied patients cited medicine shortages. However, satisfaction and stock-out were not significantly related (Pearson chi²(1) = 0.3656, p = 0.545), as 52% of respondents with good service satisfaction still reported stock-outs. Physical checks in nine health facilities revealed that 6 (55%) facilities experienced stock-outs in the past three months (Palorinya 59% and Adjumani 36%). Stockouts involved mostly Tetracycline Eye Ointment (3 facilities, 33%), Metformin, and Nifedipine (4 facilities, 44%). Causes of stock-out included inadequate supply, increased consumption due to growing refugee populations, delayed UNHCR shipments, weak logistics, and insufficient allocations from National Medical Stores. The per capita government allocation for medicine was, on average, USD 0.65, while UNHCR contributions increased this to USD 3.65 per refugee, plus 30% for host populations, which remains grossly insufficient. Supply delays, quantity discrepancies, and non-functional inventory systems were also observed, highlighting critical gaps in medicine availability and logistics management.
Economic Barriers to Healthcare Access for Refugees
This study found that 35% of respondents incurred out-of-pocket expenses, averaging 12,000 UGX (USD 3) per month, as shown in Figure 8 below.
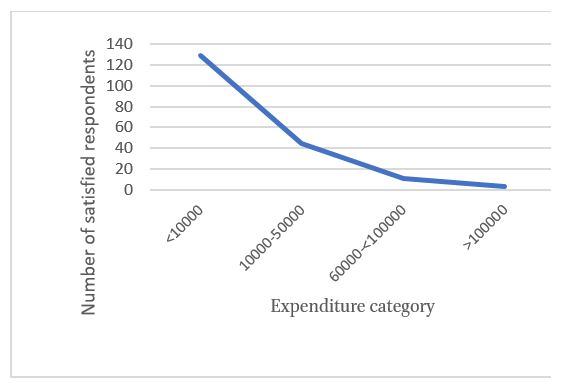
Figure 8: Variation of Service Satisfaction with Household Health Expenditure
Among the 40 respondents who spent an average of 20,000 Uganda shillings or more on health in the past three months, 28 (70%) were from Adjumani, 12 (30%) from Palorinya, and none from Palabek Settlement. Palabek is a relatively new settlement, and the refugees there are largely dependent on government- and partner-provided health services.
Income Sources Among the Refugees
Formal employment was rare in the refugee settlement, with only 4 (2%) respondents employed, and the female-to-male gender ratio was 1:2 (Figure 3 below). This means that refugees in these settlements still have very limited options to achieve self-resilience to meet the medical costs not included in the Uganda National Minimum Health Package.
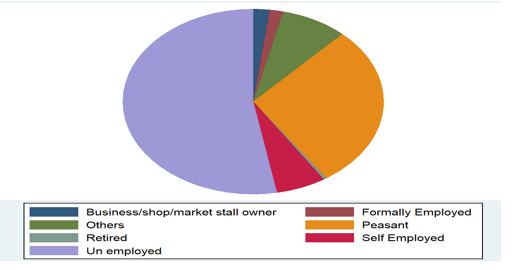
Figure 9: Employment Status of Respondents
The informal sector employed 29% in subsistence agriculture and 16% in other activities. Agriculture showed no significant gender disparity and was most common in Palorinya. Refugees have access to small plots (30×30 m), while renting additional land from host communities (~USD 30/acre/year) is largely unaffordable. Limited funding and withdrawal of livelihood partners further constrained opportunities for agricultural engagement.
Sources of income were small-scale agriculture (50%), WFP (27%), small businesses (10%), families and friends in Uganda (9%), and foreign remittances (3%). Multipurpose from partners constituted only 1%. The average monthly household income of employed refugees was too meager to support their families, as shown in Figure 10 below.
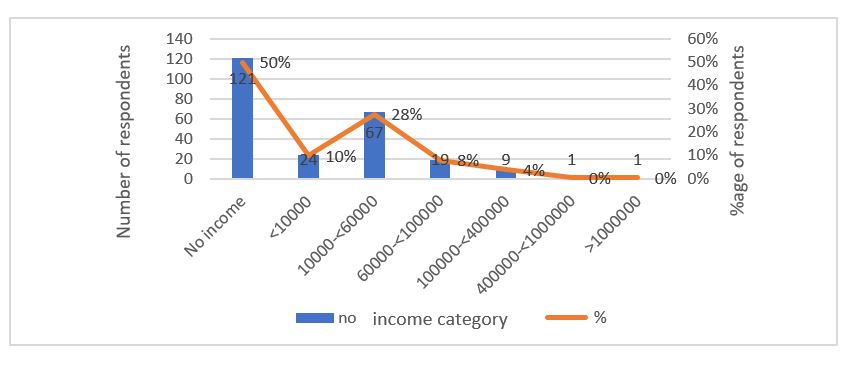
Figure 10: Average Income per Month Among the Respondents
The study highlights the prevalence of extreme poverty among refugees in the study area. An average monthly income of UGX 60,000 provides only about USD 0.6 per day for an entire household, or USD 0.1 per person per day in an average family of five, even before other basic needs are considered. Ongoing WFP food rationing and exclusion from food assistance further worsen food and nutrition insecurity, undermining health. Compared with the international poverty line of USD 3 per person per day, a refugee family (with an average family size of 5 people) would require USD 15 daily but survives on about USD 0.5, which is more than 30 times below the international Poverty Line.
There is an urgent need for economic empowerment interventions, including livelihood support, market linkages, land access, and improved agricultural technologies.
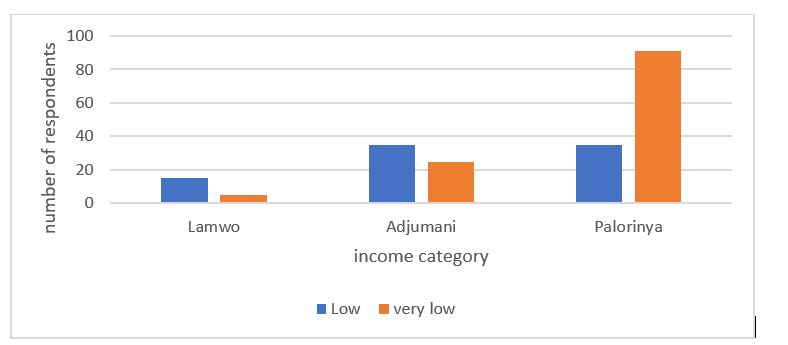
Figure 11: Income Distribution Among the Respondents
This study found that staffing levels in refugee settlement health facilities averaged 56% of the Ministry of Health’s revised norms, with a health worker density (HWD) of 2.1/1000 population, which is well below the WHO-recommended level of 4.45/1000. Duty attendance was similarly low (56%), with overall absenteeism at 44% (13% authorized, 31% unauthorized), limiting functional healthcare access for refugees and host communities. Higher-level facilities, including Moyo District Hospital, had the lowest staffing levels.
Payroll management remains fragmented, with only 38% of staff on the government payroll and the rest on partner payrolls, resulting in parallel systems with differing terms of employment. Governance and leadership gaps were evident: the Reward and Sanction Committees underperformed, and four facilities had dual in-charges, resulting in conflicts over duty rosters and leave schedules.
5. Discussion
5.1. Policy-Practice Gap in the Integration Process
Uganda’s progressive legal framework for refugee protection, anchored in the Constitution of the Republic of Uganda, the Refugee Act (2006), and the Refugee Regulations (2010), ensures refugees equal access to public services. These policies are operationalized through sector-specific plans, such as the Health Sector Integrated Refugee Response Plan (2019–2024), which integrates refugee health into district planning and aligns with the Global Compact on Refugees and WHO guidelines on integrating migrants into national health systems.
Despite this robust legal foundation, this study identified a substantial policy-practice gap at the frontline level. Up to 50% of health facility in-charges were unaware of policies governing refugees’ entitlements, potentially undermining effective service delivery. In Uganda, health facility in-charges play a central role in planning, delivering, and monitoring health services. A lack of awareness among these frontline managers can directly limit refugees’ access to services, highlighting weaknesses in health governance and leadership, a key pillar of the healthcare system. According to systems theory, inefficiencies in one pillar of a health system affect the system’s overall functioning, reducing equity, efficiency, and sustainability. Similar policy-practice gaps have been documented in Southern Africa and Europe, emphasizing that progressive laws alone are insufficient without proper dissemination, capacity building, and operationalization.
5.2 Local Integration and Participation
The study revealed strong social integration between refugees and host communities but weak social links between refugees and government authorities. Only 22% of respondents reported having been consulted on health or community development planning. Weak social links constrain integration across other sectors, including livelihoods, education, and governance, demonstrating that health integration alone is insufficient. The social determinants of health, including access to livelihoods, security, education, water, and sanitation, have a significant impact on health outcomes. Without meaningful integration in these sectors, health service integration is likely to be fragmented and unsustainable. Inclusion of refugees in governance structures fosters dignity, ownership, accountability, cost-effectiveness, and long-term sustainability of health interventions.
5.3 Health Service Utilization, Trust, and Satisfaction
Financial constraints largely dictated refugees’ reliance on government health facilities, as nearly 50% had no income sources and thus had limited ability to access private clinics. The UNMHCP provides a minimum package of free health services; however, services beyond this package incur direct costs. About 12% of respondents expressed dissatisfaction with government services, yet returned due to a lack of alternatives. Mental health services and care for the disabled and elderly remain under-prioritized, consistent with global trends in resource-constrained refugee settings.
5.4 Human Resources
The low staffing level, with consultations per clinician per day exceeding 80, recorded in this study, exacerbates staff stress and turnover. Delays in implementing revised staffing norms and poor working conditions discourage retention, with nearly 45% of Ugandan medical students intending to work outside the national health system. Staff absenteeism further undermines service delivery, cost-effectiveness, and sustainability. The biometric attendance system has shown promise in reducing absenteeism, suggesting scalable solutions that can be implemented.
5.5 Health Financing, Livelihoods, and Economic Barriers
Uganda allocates approximately 7% of its national budget to health, which is below the Abuja Declaration target of 15%. Although primary health care is officially free, refugees incur hidden costs for transportation and medicines not covered by UNMHCP. Only 2% of respondents had formal employment, with low monthly incomes averaging USD 17. Out-of-pocket health expenditures ranged from 12,000 to 30,000 Uganda shillings per month, often exceeding 40% of non-subsistence income, meeting WHO criteria for catastrophic expenditure. Livelihood programming has drastically reduced, and only 1% accessed multipurpose cash grants, trapping them in a cycle of poverty and inadequate healthcare access. Economic empowerment interventions, including conditional cash transfers, multipurpose grants, and livelihood programs, are critical for improving functional healthcare access.
5.6 Governance, Participation, and Sustainability
Governance gaps, including dual leadership structures, parallel payrolls, and weak accountability mechanisms, have limited the effectiveness of the health system. Refugees’ representation in Health Unit Management Committees (HUMC) was limited, undermining inclusion and ownership. Fragmented governance increases costs, reduces efficiency, and threatens the long-term sustainability of refugee health integration. Harmonization of payroll systems, leadership structures, and meaningful participation by refugees are prerequisites for resilient, cost-effective healthcare integration.
5.7 Policy Implications and Recommendations for IGOs
Short-Term (Operational and Policy Level):
- Disseminate refugee health policies and provide targeted capacity building for frontline staff.
- Deploy interpreters from refugee communities and develop multilingual health education materials.
Medium Term (Systemic and Strategic Level):
- Strengthen medicine supply chains, improve inventory management.
- Attract, motivate, and retain health workers through temporary staffing, incentives, and biometric attendance monitoring.
- Enhance refugees’ participation in health governance.
- Implement livelihood interventions, cash transfers, and subsidies to reduce catastrophic out-of-pocket expenditures.
Long-Term (Systemic and Strategic Level):
7. Harmonize refugee and national health governance structures, eliminating parallel systems.
6. Reform health financing, including integration of refugees in a National Health Insurance Scheme.
7. Integrate health with other sectors to address social determinants, ensuring multisectoral refugee inclusion.
8. Invest in resilient supply chains, infrastructure, and digital health logistics platforms.
9. Fully integrate refugee health data into the national information system (DHIS2) for evidence-based planning.
6. Conclusion
Uganda’s progressive refugee legal framework, a global best practice in solidarity and resilience, remains fragile and largely unsustainable. Long-term sustainability requires bridging policy-practice gaps, strengthening governance, improving financing, ensuring refugees’ participation and global collaboration.
7. Acknowledgments:
I acknowledge the review team for their guidance and feedback during this manuscript development.
- Conflict of Interest Statement
The author states that there is no conflict of interest.
9 References
Aceng, Dr Jane Ruth. HEALTH SECTOR MINISTERIAL POLICY STATEMENT. n.d.
Adesina, Miracle, Muhammad Adeel, Olamide Omigbile, et al. ‘Trends and Drivers of Refugees in Africa’. European Journal of Environment and Public Health 6, no. 1 (2021): em0093. https://doi.org/10.21601/ejeph/11379.
Adesina, Miracle, Muhammad Adeel, Olamide Omigbile, et al. ‘Trends and Drivers of Refugees in Africa’. European Journal of Environment and Public Health 6, no. 1 (2021): em0093. https://doi.org/10.21601/ejeph/11379.
‘Age Dependency Ratio (% of Working-Age Population) – Uganda | Data’. Accessed 20 October 2025. https://data.worldbank.org/indicator/SP.POP.DPND?locations=UG.
Ager, A., and A. Strang. ‘Understanding Integration: A Conceptual Framework’. Journal of Refugee Studies 21, no. 2 (2008): 166–91. https://doi.org/10.1093/jrs/fen016.
Ager, A., and A. Strang. ‘Understanding Integration: A Conceptual Framework’. Journal of Refugee Studies 21, no. 2 (2008): 166–91. https://doi.org/10.1093/jrs/fen016.
Alfaro-Velcamp, Theresa. ‘“Don’t Send Your Sick Here to Be Treated, Our Own People Need It More”: Immigrants’ Access to Healthcare in South Africa’. International Journal of Migration, Health and Social Care 13, no. 1 (2017): 53–68. https://doi.org/10.1108/IJMHSC-04-2015-0012.
A/RES/71/1: New York Declaration for Refugees and Migrants. n.d.
A/RES/71/1: New York Declaration for Refugees and Migrants. n.d.
Atiga, Oswald, Jackie Walters, and Noleen Pisa. ‘Challenges of Medical Commodity Availability in Public and Private Health Care Facilities in the Upper East Region of Ghana: A Patient-Centered Perspective’. BMC Health Services Research 23, no. 1 (2023): 719. https://doi.org/10.1186/s12913-023-09717-9.
Atrafi, Hélène. Working towards Inclusion – Refugees within the National Systems of Ethiopia. n.d.
Biggam, John. Succeeding with Your Master’s Dissertation: A Step-by-Step Handbook. McGraw Hill/Open University Press, 2010.
Bingham, Andrea J. ‘From Data Management to Actionable Findings: A Five-Phase Process of Qualitative Data Analysis’. International Journal of Qualitative Methods 22 (October 2023): 16094069231183620. https://doi.org/10.1177/16094069231183620.
Böhret, Ines. Absenteeism of Health Workers in Uganda. 2018. https://doi.org/10.13140/RG.2.2.11896.90886.
Böhret, Ines. Absenteeism of Health Workers in Uganda. 2018. https://doi.org/10.13140/RG.2.2.11896.90886.
Borkowski, Artur, Lily Calaycay, and Bindu Sunny. Paving Pathways for Inclusion: 3 Levers Countries Can Use to Include Refugees in Education Systems. 2024.
Borkowski, Artur, Lily Calaycay, and Bindu Sunny. Paving Pathways for Inclusion: 3 Levers Countries Can Use to Include Refugees in Education Systems. n.d.
Borkowski, Artur, Lily Calaycay, and Bindu Sunny. Paving Pathways for Inclusion: 3 Levers Countries Can Use to Include Refugees in Education Systems. n.d.
Boyce, Carolyn, and Palena Neale. CONDUCTING IN-DEPTH INTERVIEWS: 2006.
Brandenberger, Julia, Thorkild Tylleskär, Katrin Sontag, Bernadette Peterhans, and Nicole Ritz. ‘A Systematic Literature Review of Reported Challenges in Health Care Delivery to Migrants and Refugees in High-Income Countries – the 3C Model’. BMC Public Health 19, no. 1 (2019): 755. https://doi.org/10.1186/s12889-019-7049-x.
Brandenberger, Julia, Thorkild Tylleskär, Katrin Sontag, Bernadette Peterhans, and Nicole Ritz. ‘A Systematic Literature Review of Reported Challenges in Health Care Delivery to Migrants and Refugees in High-Income Countries – the 3C Model’. BMC Public Health 19, no. 1 (2019): 755. https://doi.org/10.1186/s12889-019-7049-x.
‘Budget Speech FY 2024-25.Pdf’. n.d. Accessed 22 September 2025. https://budget.finance.go.ug/sites/default/files/National%20Budget%20docs/Budget%20Speech%20FY%202024-25.pdf?utm_source=chatgpt.com.
Chiarenza, Antonio, Marie Dauvrin, Valentina Chiesa, Sonia Baatout, and Hans Verrept. ‘Supporting Access to Healthcare for Refugees and Migrants in European Countries under Particular Migratory Pressure’. BMC Health Services Research 19, no. 1 (2019): 513. https://doi.org/10.1186/s12913-019-4353-1.
Chuah, Fiona Leh Hoon, Sok Teng Tan, Jason Yeo, and Helena Legido-Quigley. ‘Health System Responses to the Health Needs of Refugees and Asylum-Seekers in Malaysia: A Qualitative Study’. International Journal of Environmental Research and Public Health 16, no. 9 (2019): 1584. https://doi.org/10.3390/ijerph16091584.
Common Health Needs of Refugees and Migrants: Literature Review. 1st ed. World Health Organization, 2021.
Coumans, J. V. F., and S. Wark. ‘A Scoping Review on the Barriers to and Facilitators of Health Services Utilisation Related to Refugee Settlement in Regional or Rural Areas of the Host Country’. BMC Public Health 24, no. 1 (2024): 199. https://doi.org/10.1186/s12889-024-17694-9.
Coumans, J. V. F., and S. Wark. ‘A Scoping Review on the Barriers to and Facilitators of Health Services Utilisation Related to Refugee Settlement in Regional or Rural Areas of the Host Country’. BMC Public Health 24, no. 1 (2024): 199. https://doi.org/10.1186/s12889-024-17694-9.
Crane, Lani, Naomi Blumberg, Miguel Pulido, Paulina Giusti, Ana Ragonesi, Andrea Ortiz, and Ricardo Chuquimia Vidal. Integrating and Including Migrants in National Health Systems. 2024.
Crane, Lani, Naomi Blumberg, Miguel Pulido, Paulina Giusti, Ana Ragonesi, Andrea Ortiz, and Ricardo Chuquimia Vidal. Integrating and Including Migrants in National Health Systems. n.d.
Crane, Lani, Naomi Blumberg, Miguel Pulido, Paulina Giusti, Ana Ragonesi, Andrea Ortiz, and Ricardo Chuquimia Vidal. Integrating and Including Migrants in National Health Systems. n.d.
Crawford, Nicholas, and Sorcha O’Callaghan. The Comprehensive Refugee Response Framework. n.d.
Crisp, Jeff. A New Asylum Paradigm? Globalization, Migration and the Uncertain Future of the International Refugee Regime. n.d.
Crisp, Jeff. A New Asylum Paradigm? Globalization, Migration and the Uncertain Future of the International Refugee Regime. n.d.
Dadzie, Gertrude Morgan. Healthcare Accessibility for Syrian Refugees: Understanding Trends, Host Countries’ Responses and Impacts on Refugees’ Health. n.d.
‘Delivering Emergency Health and Nutrition Services to Refugees in Kenya and Ethiopia’. Accessed 20 October 2025. https://documents.worldbank.org/en/publication/documents-reports/documentdetail/342151468001153494.
Ebrahim, Nader Ale. Approach to Conduct an Effective Literature Review. n.d.
Eeuwijk, Peter van, and Zuzanna Angehrn. How to … Conduct a Focus Group Discussion (FGD). n.d.
Elnakib, Shatha, Laila Akhu-Zaheya, Wejdan Khater, et al. ‘The Emergence and Regression of Political Priority for Refugee Integration into the Jordanian Health System: An Analysis Using the Kingdon’s Multiple Streams Model’. Conflict and Health 18, no. S1 (2024): 30. https://doi.org/10.1186/s13031-024-00588-3.
Elnakib, Shatha, Caitlin Jackson, Ummekulsoom Lalani, Yusra Ribhi Shawar, and Sara Bennett. ‘How Integration of Refugees into National Health Systems Became a Global Priority: A Qualitative Policy Analysis’. Conflict and Health 18, no. S1 (2024): 31. https://doi.org/10.1186/s13031-024-00587-4.
‘Evaluation of the Implementation of the Global Compact on Refugees and Its Comprehensive Refugee Response Framework (CRRF) in Uganda: Evaluation Report – Google Search’. Accessed 20 October 2025. https://www.google.com/search?q=Evaluation+of+the+implementation+of+the+Global+Compact+on+Refugees+and+its+Comprehensive+Refugee+Response+Framework.
Feldman, R. ‘Primary Health Care for Refugees and Asylum Seekers: A Review of the Literature and a Framework for Services’. Public Health 120, no. 9 (2006): 809–16. https://doi.org/10.1016/j.puhe.2006.05.014.
‘Fiscal_decentralization_fellows_paper.Pdf’. n.d. Accessed 8 October 2025. https://www.undp.org/sites/g/files/zskgke326/files/2025-01/fiscal_decentralization_fellows_paper.pdf.
Forman, Lisa, and Dr Diya Uberoi. Uganda National Health Insurance BASED ON A PAPER PREPARED FOR CEHURD BY: n.d.
Foster, Elizabeth, Dean Jolliffe, Gabriel Lara Ibarra, Christoph Lakner, and Samuel Tetteh-Baah. Global Poverty Revisited Using 2021 PPPs and New Data on Consumption. n.d.
Global Trends | UNHCR. n.d.
Haynie, Deson. Models of Refugee Health Care. n.d.
Haynie, Deson. Models of Refugee Health Care. n.d.
Health and Nutrition Service Provision for Refugees and Asylum Seekers in Ethiopia. n.d.
Health and Nutrition Service Provision for Refugees and Asylum Seekers in Ethiopia. n.d.
‘Health Insurance for Refugees in Rwanda, Pdf – Google Search’. Accessed 8 October 2025. https://www.google.com/search?q=health+insurance+for+refugees+in+Rwanda.
‘Health-Alternative-Policy-Statement-FY2025-26.Pdf’. n.d. Accessed 21 August 2025. https://parliamentwatch.ug/wp-content/uploads/2025/03/Health-Alternative-Policy-Statement-FY2025-26.pdf.
‘Healthcare-Explainer.Pdf’. n.d. Accessed 20 October 2025. https://scalabrini.org.za/wp-content/uploads/2019/09/Healthcare-Explainer.pdf.
‘Health-Care-Systems-1.Pdf’. n.d. Accessed 7 August 2025. https://thecitizenreport.ug/wp-content/uploads/2022/05/Health-Care-Systems-1.pdf.
Healthy Lives: Top Ten Operations by Expenditure. n.d.
Huddleston, Written Thomas, Jan Niessen, and Jasper Dag Tjaden. Using EU Indicators of Immigrant Integration. n.d.
Hynie, Michaela. ‘Refugee Integration: Research and Policy.’ Peace and Conflict: Journal of Peace Psychology 24, no. 3 (2018): 265–76. https://doi.org/10.1037/pac0000326.
Hynie, Michaela. ‘Refugee Integration: Research and Policy.’ Peace and Conflict: Journal of Peace Psychology 24, no. 3 (2018): 265–76. https://doi.org/10.1037/pac0000326.
Jackson, Claire L., Deborah A. Askew, Caroline Nicholson, and Peter M. Brooks. ‘The Primary Care Amplification Model: Taking the Best of Primary Care Forward’. BMC Health Services Research 8, no. 1 (2008): 268. https://doi.org/10.1186/1472-6963-8-268.
Joshi, Chandni, Grant Russell, I.-Hao Cheng, et al. ‘A Narrative Synthesis of the Impact of Primary Health Care Delivery Models for Refugees in Resettlement Countries on Access, Quality and Coordination’. International Journal for Equity in Health 12, no. 1 (2013): 88. https://doi.org/10.1186/1475-9276-12-88.
Joshi, Chandni, Grant Russell, I.-Hao Cheng, et al. ‘A Narrative Synthesis of the Impact of Primary Health Care Delivery Models for Refugees in Resettlement Countries on Access, Quality and Coordination’. International Journal for Equity in Health 12, no. 1 (2013): 88. https://doi.org/10.1186/1475-9276-12-88.
Jowett, Matthew, Maria Petro Brunal, Gabriela Flores, and Jonathan Cylus. Spending Targets for Health: No Magic Number. n.d.
Kay, Margaret, Claire Jackson, and Caroline Nicholson. ‘Refugee Health: A New Model for Delivering Primary Health Care’. Australian Journal of Primary Health 16, no. 1 (2010): 98. https://doi.org/10.1071/PY09048.
Kay, Margaret, Claire Jackson, and Caroline Nicholson. ‘Refugee Health: A New Model for Delivering Primary Health Care’. Australian Journal of Primary Health 16, no. 1 (2010): 98. https://doi.org/10.1071/PY09048.
Kohlenberger, Judith, Isabella Buber-Ennser, Bernhard Rengs, Sebastian Leitner, and Michael Landesmann. ‘Barriers to Health Care Access and Service Utilization of Refugees in Austria: Evidence from a Cross-Sectional Survey’. Health Policy 123, no. 9 (2019): 833–39. https://doi.org/10.1016/j.healthpol.2019.01.014.
Kohlenberger, Judith, Isabella Buber-Ennser, Bernhard Rengs, Sebastian Leitner, and Michael Landesmann. ‘Barriers to Health Care Access and Service Utilization of Refugees in Austria: Evidence from a Cross-Sectional Survey’. Health Policy 123, no. 9 (2019): 833–39. https://doi.org/10.1016/j.healthpol.2019.01.014.
Komakech, Henry, Evelyn Baelvina Nyachwo, and David Lubogo. ‘Integrated Health Services for Refugee and Host Populations in Uganda: A Qualitative Study of Stakeholder’s Perspectives’. Global Public Health 19, no. 1 (2024): 2387445. https://doi.org/10.1080/17441692.2024.2387445.
Konde-Lule, Joseph, Sheba N. Gitta, Anne Lindfors, Sam Okuonzi, Virgil On Onama, and Birger C. Forsberg. ‘Private and Public Health Care in Rural Areas of Uganda’. BMC International Health and Human Rights 10, no. 1 (2010): 29. https://doi.org/10.1186/1472-698X-10-29.
Lebano, Adele, Sarah Hamed, Hannah Bradby, et al. ‘Migrants’ and Refugees’ Health Status and Healthcare in Europe: A Scoping Literature Review’. BMC Public Health 20, no. 1 (2020): 1039. https://doi.org/10.1186/s12889-020-08749-8.
Lugada, Eric, Irene Ochola, Anthony Kirunda, et al. ‘Health Supply Chain System in Uganda: Assessment of Status and of Performance of Health Facilities’. Journal of Pharmaceutical Policy and Practice 15, no. 1 (2022): 58. https://doi.org/10.1186/s40545-022-00452-w.
Lugada, Eric, Irene Ochola, Anthony Kirunda, et al. ‘Health Supply Chain System in Uganda: Assessment of Status and of Performance of Health Facilities’. Journal of Pharmaceutical Policy and Practice 15, no. 1 (2022): 58. https://doi.org/10.1186/s40545-022-00452-w.
Mangrio, Elisabeth, and Katarina Sjögren Forss. ‘Refugees’ Experiences of Healthcare in the Host Country: A Scoping Review’. BMC Health Services Research 17, no. 1 (2017): 814. https://doi.org/10.1186/s12913-017-2731-0.
Mangrio, Elisabeth, and Katarina Sjögren Forss. ‘Refugees’ Experiences of Healthcare in the Host Country: A Scoping Review’. BMC Health Services Research 17, no. 1 (2017): 814. https://doi.org/10.1186/s12913-017-2731-0.
Mapping Health Systems’ Responsiveness to Refugee and Migrant Health Needs. 1st ed. World Health Organization, 2021.
Mapping Health Systems’ Responsiveness to Refugee and Migrant Health Needs. 1st ed. World Health Organization, 2021.
Medard, Turyamureba, Bruno L. Yawe, and Oryema John Bosco. ‘Health Care Delivery System in Uganda: A Review’. Tanzania Journal of Health Research, n.d.
Medard, Turyamureba, Bruno L. Yawe, and Oryema John Bosco. ‘Health Care Delivery System in Uganda: A Review’. Tanzania Journal of Health Research, n.d.
Meyer-Weitz, Anna, Kwaku Oppong Asante, and Bukenge J. Lukobeka. ‘Healthcare Service Delivery to Refugee Children from the Democratic Republic of Congo Living in Durban, South Africa: A Caregivers’ Perspective’. BMC Medicine 16, no. 1 (2018): 163. https://doi.org/10.1186/s12916-018-1153-0.
Mid-Year Trends | UNHCR. n.d.
Migrant and Refugee Access to Public Healthcare in South Africa – Scalabrini. n.d.
Mitchell, Andrew. Strategic Approaches for Refugee Inclusion in Social Protection Systems. n.d.
Mitchell, Andrew. Strategic Approaches for Refugee Inclusion in Social Protection Systems. n.d.
Mohammadi, Soheila, Aje Carlbom, Robabeh Taheripanah, and Birgitta Essén. ‘Experiences of Inequitable Care among Afghan Mothers Surviving Near-Miss Morbidity in Tehran, Iran: A Qualitative Interview Study’. International Journal for Equity in Health 16, no. 1 (2017): 121. https://doi.org/10.1186/s12939-017-0617-8.
Mohammadi, Soheila, Aje Carlbom, Robabeh Taheripanah, and Birgitta Essén. ‘Experiences of Inequitable Care among Afghan Mothers Surviving Near-Miss Morbidity in Tehran, Iran: A Qualitative Interview Study’. International Journal for Equity in Health 16, no. 1 (2017): 121. https://doi.org/10.1186/s12939-017-0617-8.
Nabyonga Orem, J., F. Mugisha, C. Kirunga, J. Macq, and B. Criel. ‘Abolition of User Fees: The Uganda Paradox’. Health Policy and Planning 26, no. Suppl. 2 (2011): ii41–51. https://doi.org/10.1093/heapol/czr065.
NPHC 2024 – Preliminary Results. 2024.
NPHC 2024 – Preliminary Results. 2024.
NPHC 2024 – Preliminary Results. 2024.
Olaniran, Abimbola, Jane Briggs, Ami Pradhan, et al. ‘Stock-Outs of Essential Medicines among Community Health Workers (CHWs) in Low- and Middle-Income Countries (LMICs): A Systematic Literature Review of the Extent, Reasons, and Consequences’. Human Resources for Health 20, no. 1 (2022): 58. https://doi.org/10.1186/s12960-022-00755-8.
Olaniran, Abimbola, Jane Briggs, Ami Pradhan, et al. ‘Stock-Outs of Essential Medicines among Community Health Workers (CHWs) in Low- and Middle-Income Countries (LMICs): A Systematic Literature Review of the Extent, Reasons, and Consequences’. Human Resources for Health 20, no. 1 (2022): 58. https://doi.org/10.1186/s12960-022-00755-8.
O.Nyumba, Tobias, Kerrie Wilson, Christina J. Derrick, and Nibedita Mukherjee. ‘The Use of Focus Group Discussion Methodology: Insights from Two Decades of Application in Conservation’. Methods in Ecology and Evolution 9, no. 1 (2018): 20–32. https://doi.org/10.1111/2041-210X.12860.
Otieno, Emmanuel, and Josephine Namyalo. ‘The Paradox of the Ugandan Health Insurance System: Challenges and Opportunities for Health Reform’. Journal of Preventive Medicine and Public Health 57, no. 1 (2024): 91–94. https://doi.org/10.3961/jpmph.23.110.
Otieno, Emmanuel, and Josephine Namyalo. ‘The Paradox of the Ugandan Health Insurance System: Challenges and Opportunities for Health Reform’. Journal of Preventive Medicine and Public Health 57, no. 1 (2024): 91–94. https://doi.org/10.3961/jpmph.23.110.
Out-of-Pocket Expenditure (% of Current Health Expenditure) – Iran, Islamic Rep. | Data. n.d.
Out-of-Pocket Expenditure (% of Current Health Expenditure) – Iran, Islamic Rep. | Data. n.d.
- Iqbal, Maha, Ramesh Walpola, Ben Harris‐Roxas, et al. ‘Improving Primary Health Care Quality for Refugees and Asylum Seekers: A Systematic Review of Interventional Approaches’. Health Expectations 25, no. 5 (2022): 2065–94. https://doi.org/10.1111/hex.13365.
Polglase, Katie. Health Sector Humanitarian Response Strategy. 2015.
Polglase, Katie. Health Sector Humanitarian Response Strategy. 2015.
‘Policy-Analysis-Triangle-Adapted-from-Walt-and-Gilson-1994-Detailed-Legends-The.Png (339×176)’. n.d. Accessed 8 October 2025. https://www.researchgate.net/publication/280030454/figure/fig1/AS:267559702364183@1440802612162/Policy-analysis-triangle-adapted-from-Walt-and-Gilson-1994-Detailed-legends-The.png.
‘Poverty and Equity Profile Uganda’. n.d. Accessed 7 October 2025. https://documents1.worldbank.org/curated/en/099523204222530354/pdf/IDU-30f95e03-7d91-400b-a4a5-d68c284d6f97.pdf.
Report: Promoting Refugees Right. 2, no. 4 (2016).
Russell, Grant, Mark Harris, I.-Hao Cheng, et al. Coordinated Primary Health Care for Refugees: A Best Practice Framework for Australia. n.d.
Santric-Milicevic, Milena, Milena Vasic, Vladimir Vasic, et al. ‘Uptake of Health Care Services by Refugees: Modelling a Country Response to a Western Balkan Refugee Crisis’. Healthcare 8, no. 4 (2020): 560. https://doi.org/10.3390/healthcare8040560.
Santric-Milicevic, Milena, Milena Vasic, Vladimir Vasic, et al. ‘Uptake of Health Care Services by Refugees: Modelling a Country Response to a Western Balkan Refugee Crisis’. Healthcare 8, no. 4 (2020): 560. https://doi.org/10.3390/healthcare8040560.
Sebba, Kalyango Ronald. Land Conflicts and Their Impact on Refugee Women’s Livelihoods in Southwestern Uganda. n.d.
Selcuk, Besir Demi, and Nuray Pismek. ‘Convergent Parallel Mixed-Methods Study of Controversial Issues in Social Studies Classes: A Clash of Ideologies’. Educational Sciences: Theory & Practice, ahead of print, 2018. https://doi.org/10.12738/estp.2018.1.0298.
Sherif, Bafreen, Ahmed Awaisu, and Nadir Kheir. ‘Refugee Healthcare Needs and Barriers to Accessing Healthcare Services in New Zealand: A Qualitative Phenomenological Approach’. BMC Health Services Research 22, no. 1 (2022): 1310. https://doi.org/10.1186/s12913-022-08560-8.
Spahl, Wanda, and August Österle. ‘Stratified Membership: Health Care Access for Urban Refugees in Turkey’. Comparative Migration Studies 7, no. 1 (2019): 42. https://doi.org/10.1186/s40878-019-0148-0.
Spitzer, Denise L., Sara Torres, Anthony B. Zwi, Ernest Nene Khalema, and Erlinda Palaganas. ‘Towards Inclusive Migrant Healthcare’. BMJ, 16 September 2019, l4256. https://doi.org/10.1136/bmj.l4256.
Stanciole, Anderson E., and Manfred Huber. Access to Health Care for Migrants, Ethnic Minorities, and Asylum Seekers in Europe. 2009.
Tafesse, Wiktoria, Julie Jemutai, Chrispus Mayora, and Federica Margini. ‘Scoping Review of Health Economics Research on Refugee Health in Sub-Saharan Africa’. Value in Health Regional Issues 39 (January 2024): 98–106. https://doi.org/10.1016/j.vhri.2023.10.008.
Tengilimoğlu, Dilaver, Aysu Zekioğlu, Fatih Budak, Hüseyin Eriş, and Mustafa Younis. ‘Refugees’ Opinions about Healthcare Services: A Case of Turkey’. Healthcare 9, no. 5 (2021): 490. https://doi.org/10.3390/healthcare9050490.
‘The Crrf Framework – Google Search’. Accessed 20 October 2025. https://www.google.com/search?q=the+crrf+framework&sca_esv=f3d4f0bd708342fc&sxsrf=AE3TifN3JRFWjCEP4E-TEHqk-
‘Uganda – Age Dependency Ratio (% Of Working-Age Population) – 2024 Data 2025 Forecast 1960-2023 Historical’. Accessed 20 October 2024. https://tradingeconomics.com/uganda/age-dependency-ratio-percent-of-working-age-population-wb-data.html.
UNHCR Uganda. ‘Guide to International Refugee Protection and Building State Asylum Systems’. n.d. https://doi.org/10.1163/2210-7975_HRD-1021-20180068.
Verguet, Stéphane, and Averi Chakrabarti. ‘Examining the Computation of the Underlying Components of DALYs’. Health Policy and Planning 38, no. 5 (2023): 648–54. https://doi.org/10.1093/heapol/czad017.
World Health Organization. Health Workforce Requirements for Universal Health Coverage and the Sustainable Development Goals. (Human Resources for Health Observer, 17). World Health Organization, 2016. https://iris.who.int/handle/10665/250330.
World Health Organization. Health Workforce Requirements for Universal Health Coverage and the Sustainable Development Goals. (Human Resources for Health Observer, 17). World Health Organization, 2016. https://iris.who.int/handle/10665/250330.
World Report on the Health of Refugees and Migrants. 1st ed. World Health Organization, 2022.
Zainal, Zaidah. Case Study as a Research Method. n.d.
Zeidan, Amy, Utsha Khatri, Michelle Munyikwa, Aba Barden, and Margaret Samuels-Kalow. ‘Barriers to Accessing Acute Care for Newly Arrived Refugees’. Western Journal of Emergency Medicine 20, no. 6 (2019): 842–50. https://doi.org/10.5811/westjem.2019.8.43129.
Zihindula, Ganzamungu, Anna Meyer-Weitz, and Olagoke Akintola. Access to Health Care Services by Refugees in Southern Africa: A Review of Literature. 16 (2015).
Zihindula, Ganzamungu, Anna Meyer-Weitz, and Olagoke Akintola. Access to Health Care Services by Refugees in Southern Africa: A Review of Literature. 16 (2015).
[1] ‘WHO -Uhl-Technical-Brief-Refugees-Migrant-Health (1)’, 2023, 1.
[2] Miracle Adesina et al., ‘Trends and Drivers of Refugees in Africa’, European Journal of Environment and Public Health 6, no. 1 (2021): 1, https://doi.org/10.21601/ejeph/11379.
[3] UNHCR Uganda, ‘Guide to International Refugee Protection and Building State Asylum Systems’, n.d., 34, https://doi.org/10.1163/2210-7975_HRD-1021-20180068.
[4] UNHCR Uganda, ‘Annual_Results_Report’, 2024, 4.
[5] NPHC 2024 – Preliminary Results, 2024, 2.
[6] ‘Annual Health Sector Performance Report 2020-21-1’, n.d., 14.
[7] ‘Poverty and Equity Profile Uganda’, n.d., 2, accessed 7 October 2025, https://documents1.worldbank.org/curated/en/099523204222530354/pdf/IDU-30f95e03-7d91-400b-a4a5-d68c284d6f97.pdf.
[8] ‘Uganda – Age Dependency Ratio (% Of Working-Age Population) – 2024 Data 2025 Forecast 1960-2023 Historical’, accessed 20 October 2024, https://tradingeconomics.com/uganda/age-dependency-ratio-%-of-working-age-population-wb-data.html.
[9] ‘Employment to Population Ratio in Uganda’, n.d.
[10] Strategic Purchasing for Primary Health Care, ‘Trend in Health Care Financing Health-Purchasing-Factsheet_Uganda READ ALready’, 2021, 4.
[11] “Health-Purchasing-Factsheet Uganda 33,” n.d., 1.
[12] Matthew Jowett et al., Spending Targets for Health: No Magic Number, n.d., 4.
[13] ‘Press-Release-Proposed-National-Health-Insurance-Bill’, n.d., 1.
[14] “Health-Purchasing-Factsheet Uganda 33,” 8.
[15] “Health Insurance for Refugees in Rwanda, Pdf – Google Search,” 2, accessed October 8, 2025, https://www.google.com/search?q=health+insurance+for+refugees+in+Rwanda%2C+pdf&sca_esv=1e4238bc8dc008dd&sxsrf=AE3Ti
[16] ‘Report of the Public Accounts Committee on the Report of the Auditor General on the Health Sector’, n.d., 19.
[17] ‘AHSPR 2019 2020’, n.d., 13.
[18] ‘BMAU Briefing Paper 15-15 – Continuous Stock-Outs of Medical Supplies in Uganda. What Are the Root Causes, n.d., 2.
[19] Oswald Atiga et al., ‘Challenges of Medical Commodity Availability in Public and Private Health Care Facilities in the Upper East Region of Ghana: A Patient-Centered Perspective’, BMC Health Services Research 23, no. 1 (2023): 13, https://doi.org/10.1186/s12913-023-09717-9.
[20] ‘Human Resources for Health Strategic Plan 2020-2030_’, n.d., 18.
[21] ‘HRH-Audit-Report-FY-2019-2020-Final (1)’, n.d., 6.
[22] Henry Komakech et al., ‘Integrated Health Services for Refugee and Host Populations in Uganda: A Qualitative Study of Stakeholder’s Perspectives’, Global Public Health 19, no. 1 (2024): 11, https://doi.org/10.1080/17441692.2024.2387445.
[23] A. Ager and A. Strang, ‘Understanding Integration: A Conceptual Framework’, Journal of Refugee Studies 21, no. 2 (2008): 170, https://doi.org/10.1093/jrs/fen016.
[24] Artur Borkowski, Lily Calaycay, and Bindu Sunny, Paving Pathways for Inclusion: 3 Levers Countries Can Use to Include Refugees in Education Systems, 2024, 2.
[25] Artur Borkowski, Calaycay, and Sunny, Paving Pathways for Inclusion: 3 Levers Countries Can Use to Include Refugees in Education Systems, 2024, 2.
[26] ‘Refugees Act 2006’, n.d., 26.



