

ABSTRACT
| Kaduna State in northern Nigeria has experienced recurrent Lassa fever outbreaks, with rising morbidity and mortality over the past five years. Contributing factors include open drying of grains, storage in non-rat-proof containers, poor sanitation, rodent consumption, low health worker suspicion, inadequate infection prevention and control (IPC) practices, and low public risk perception.
A sequential explanatory mixed-methods design was used to assess healthcare workers’ awareness, knowledge, attitudes, and practices (KAP) regarding Lassa fever IPC measures, employing questionnaires, interviews, and focus group discussions. Of 398 healthcare workers sampled, 385 (99.2%) were included in the analysis. Findings revealed above-average scores in awareness (71%), knowledge (81%), attitudes (85%), practices (79%), and understanding of local and global implications (89%). Healthcare workers demonstrated good understanding of the interplay between disease, host, environment, climate, and biodiversity in Lassa fever transmission and response. Lassa fever remains a significant public health concern in Kaduna, with annual high morbidity and mortality. Effective control requires implementing recommendations including provision of PPE, water and sanitation facilities, rodent control, and well-trained, motivated healthcare workers equipped with knowledge, skills, and resources to prevent and manage outbreaks. |
|
-
Introduction
Lassa fever, a Viral Hemorrhagic Fever (VHF), is endemic in several West African countries, including Nigeria, Liberia, Sierra Leone, and Guinea.[1] [2] It is caused by the Lassa fever virus and transmitted through contact with the feces or body fluids of infected multi-mammate rats (Mastomys natalensis). It is a single-stranded ribonucleic acid (RNA) virus that was first discovered in Lassa village, Borno, Nigeria, in 1969. Seasonal outbreaks of Lassa fever are common in Low- and Middle-Income countries (LMCs) like Nigeria. An estimated 300,000-500,000 infections occur per year, with 10,000 deaths. The incubation period ranges from 5 to 21 days. About 80% of cases are asymptomatic, and 20% are associated with severe multi-systemic disease. It is a zoonotic infection, with spillovers from rats to humans and the potential for nosocomial transmission via human-to-human transmission.[3] [4] [5]
Nigeria continues to lead other nations in Lassa fever outbreaks. It poses a serious burden in endemic areas where it accounts for 6.0% of fevers, 0.7% of hospital admissions, 40% of case fatality, and almost a quarter of maternal mortality during peak periods. Lassa fever is more prevalent in southern Nigeria, with Ondo and Edo states being the most affected. Nevertheless, other states, such as Kaduna State, have also experienced Lassa fever outbreaks.[6]
Kaduna state is one of the northern states with recurrent outbreaks of Lassa fever and has witnessed rising morbidity and mortality in the last five years. These phenomena are associated with unsafe practices, such as the open drying of grains along roads, storing grains in non-rat-proof containers, poor environmental sanitation, and the hunting and consumption of rats. Other factors include a low index of suspicion of Lassa fever among healthcare workers, inadequate practice of Infection Prevention and Control (IPC) measures by healthcare workers, low compliance with IPC measures among patients and caregivers, and a low perception of risk associated with Lassa fever among the general public in Kaduna State. Currently, there are no approved vaccines for Lassa fever.[7]
Lassa fever’s early presentations can resemble those of other common tropical diseases, such as malaria and typhoid fever. Lassa fever can present with symptoms like fever, body weakness, malaise, headache, sore throat, muscle pain, chest pain, nausea, diarrhea, facial swelling, pleural effusion, and bleeding from the mouth, eyes, nose, and gastrointestinal tract. Lassa fever can lead to disabling or fatal complications; deafness occurs in 25% of patients who survive the disease, and in half of these cases, hearing returns partially after 1-3 months. In fatal cases, death usually occurs within 14 days of onset. Lassa fever is especially severe in late pregnancy, with maternal death and fetal loss occurring in greater than 80% of cases during the third trimester. Bleeding from body orifices, such as the mouth, nose, or vagina, is usually a late presentation associated with higher mortality.[8]
The diagnosis of Lassa fever can be made by Enzyme-Linked Immunosorbent Assay (ELISA), Immuno-fluorescence test (IT), Real-time Polymerase Chain Reaction (RT-PCR), virus isolation by cell culture, and post-mortem diagnosis by immuno-histochemistry on tissue. The antiviral treatment of choice is Ribavirin, in addition to symptomatic and supportive therapy with analgesics, intravenous fluids, and electrolyte management.[9]
Health workers (HCWs) are key in the epidemiological dynamics of infectious diseases (DID). They are central to the interactions between disease-causing microorganisms, environmental factors, biodiversity, patients or hosts, and climatic conditions that favor the contraction, incubation, and transmission of pathogens. Many cases of Lassa fever are presented to hospitals very late, are misdiagnosed, and do not receive the required care, leading to hospital-acquired infections and cycles of transmission and retransmission between patients and healthcare workers.[10] [11]
The health workers’ practice of infection prevention and control (IPC) measures is a critical strategy used to control and prevent Lassa fever outbreaks. Some health workers have a low index of suspicion of Lassa fever during their daily clinical activities, arising from limited knowledge of Lassa fever IPC. Inadequate practice of Lassa fever IPC endangers the lives of health workers and their patients, leading to recurrent outbreaks and avoidable morbidity and mortality.[12] [13]
Kaduna State continues to experience recurrent Lassa fever outbreaks. A previous cross-sectional study in Kaduna had established that health workers in primary and secondary health facilities in Kaduna State had poor knowledge (35.1%) of IPC.[14] The current study employs a mixed-methods design to examine health workers’ knowledge, attitudes, and practices regarding IPC in a tertiary facility.
Health workers’ knowledge of IPC measures alone cannot control Lassa fever transmission. Attitudinal disposition is key, as well as the willingness to apply knowledge in practice and follow established guidelines for managing infectious diseases, such as Lassa fever, in hospital settings. Many scholars have demonstrated that recurrent Lassa fever outbreaks are partly fueled by health workers’ failure to practice standard precautions. Strengthening training and capacity-building programs for health workers is essential in mitigating these gaps. Additionally, ensuring the steady availability and accessibility of necessary personal protective equipment (PPE) and other IPC tools is crucial in reducing the risk of Lassa fever transmission in healthcare settings.[15]
Lassa fever is primarily a preventable disease with the practice of sound environmental sanitation and personal hygiene. Government and health authorities should promote preventive measures, such as keeping food and water covered to prevent contamination by rats, storing grain and other foodstuffs in rodent-proof containers, disposing of garbage far from home, maintaining clean households, avoiding drying food materials in open places, and refraining from touching rats with bare hands.[16] [17]
Other preventive measures for Lassa fever include using Personal Protective Equipment (PPE), such as masks, gloves, goggles, and boots, during clinical and surgical procedures to reduce the risk of hospital-acquired or nosocomial infections and associated complications.[18] The prognosis of Lassa fever depends on early presentation, correct diagnosis, early commencement of treatment, and adherence to standard precautions by healthcare workers in managing cases in well-designed isolation centers with trained staff.[19]
The study addressed five (5) research questions, which aimed to uncover the depth of knowledge, perception, and behavior of healthcare workers regarding IPC practices for Lassa fever, using the sequential explanatory mixed methods design: Do health workers in Kaduna State understand the dynamics of infectious diseases (DID) and the factors driving recurrent Lassa fever outbreaks in the region; are healthcare workers (HCWs) in Kaduna State aware of the Lassa fever infection prevention and control (IPC) measures implemented in health facilities; do health workers in Kaduna State possess adequate and up-to-date knowledge of Lassa fever IPC measures; what are the attitudes of healthcare workers in Kaduna State towards implementing Lassa fever IPC measures, and do healthcare workers in Kaduna State effectively practice Lassa fever IPC measures, and what barriers hinder compliance?
- Infectious Diseases
Pathogens are disease-causing microorganisms that interfere with the normal physiologic functions of the cells and tissues. Diseases have plagued man for thousands of years. Disease and infection are constant features of man’s evolution and have defined and shaped humanity’s existence, from the ravage of bubonic plague or black death in the Dark Ages to the challenges of emerging and reemerging diseases of Lassa fever, Ebola, and COVID-19. The population, at one point, succumbs to a ravaging infection, leaving deaths and sorrows in its wake.[20] .[21]
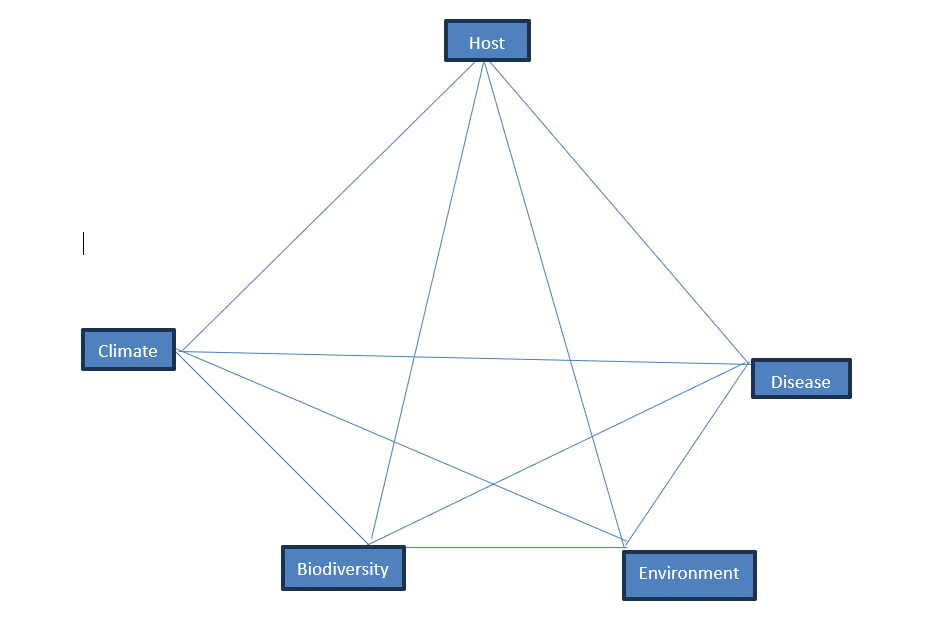
Figure 1: Conceptual Framework- Dynamics of Infectious Diseases[22]
2.1. Infection Prevention and Control (IPC)
Prevention and control efforts can happen at both the individual and population levels. The IPC conceptual framework, adapted from previous work on protocol for a systematic review of economic analyses of nosocomial infection prevention and control interventions in OECD hospitals, remains relevant in conceptualizing Lassa fever IPC measures in under-resource settings like Nigeria.[23] At the individual level, prevention efforts fall into two categories: avoiding the contraction of infectious agents and preventing the further spread of an agent. Effective prevention depends on a solid understanding of the transmission dynamics of a particular infectious agent. Hand washing, for example, helps prevent Lassa Fever and many gastrointestinal diseases. Treatment efforts can have many different goals. It is to help the infected person feel better, cure the infection, and reduce the infection’s ability to spread. In reality, we often do not have treatments that can achieve all three of these goals simultaneously. For example, some diseases cannot be cured. In other situations, some treatments that are used to cure infections have uncomfortable side effects.[24] Public health scholars have explored healthcare workers’ knowledge, attitudes, and practices in nosocomial infection prevention and control, in relation to the barriers and enablers of IPC protocol compliance, and found that healthcare workers are critical in implementing IPC measures.[25] Vaccination is one of the most cost-effective measures for preventing and controlling infections, and it has saved lives and promoted healthy livelihoods worldwide. However, there are no vaccines for Lassa fever. Environmental sanitation and personal hygiene are the primary foundations for prevention and control.[26]
Other preventive measures for Lassa fever include using Personal Protective Equipment (PPE), such as masks, gloves, goggles, and boots, during clinical and surgical procedures to reduce the risk of hospital-acquired or nosocomial infections and associated complications. In addition, hospitals and health facilities should be designed to promote good ventilation, provide facilities for hand washing (before and after touching patients or their materials or during ward rounds), implement effective procedures, maintain sanitation, and isolate very sick patients from other patients. Clinicians and caregivers should avoid contact with blood and body fluids when caring for individuals who are ill.[27] [28] [29]
Lassa fever is a Viral Hemorrhagic Fever (VHF) infection prevalent in Nigeria, with recurrent seasonal outbreaks and high mortality and morbidity rates in certain parts of the country. It is a single-stranded RNA virus, first discovered in Lassa village, Borno, Nigeria, in 1969.[30]
Lassa Fever is one of the emerging diseases with a high mortality of >50% among hospitalized patients. It causes enormous morbidity and accounts for high Disability Adjusted Life Years (DALYs) in at-risk communities in Nigeria and other West African countries.[31] Lassa fever is an acute viral hemorrhagic illness caused by the Lassa virus, a member of the Arenavirus family, which is transmitted by the multimammate rat (Mastomys natalensis) through bites or contact with their blood or body fluids.[32]
It is endemic in countries of West Africa, including Nigeria, Liberia, Sierra Leone, and Guinea. An estimated 300,000-500,000 infections occur per year, with 10,000 deaths. The three states of Bauchi, Edo, and Ondo account for a significant portion of Nigeria’s Lassa fever burden. The Incubation period ranges from 5 to 21 days. About 80% of cases are asymptomatic, and 20% are associated with severe multi-systemic disease. It is a zoonotic infection, with spillovers from rats to humans and the potential for nosocomial outbreaks via human-to-human transmission.[33] [34] [35]
It has two modes of transmission: rodent-to-human and human-to-human. Rodent-to-human transmission occurs through the ingestion of food or materials contaminated by infected rodent excreta or urine, the handling and preparation of Mastomys as a food source, and the inhalation of aerosolized viruses..[36] [37]
Lassa fever is common among hunters and farmers who are regularly exposed to rats or working in fields contaminated by rats’ feces and urine. Health workers also risk contracting Lassa fever during routine clinical work and surgical procedures. It is more prevalent during the dry season and harvest, when grains and farm produce are often left to dry open on farms or along roads.[38]
Lassa fever can present with symptoms like fever, body weakness, malaise, headache, sore throat, muscle pain, chest pain, nausea, diarrhea, facial swelling, pleural effusion, and bleeding from the mouth, eyes, nose, and gastrointestinal tract. Lassa fever can lead to disabling or fatal complications; deafness occurs in 25% of patients who survive the disease, and in half of these cases, hearing returns partially after 1-3 months. In fatal cases, death usually occurs within 14 days of onset. Lassa fever is especially severe in late pregnancy, with maternal death and fetal loss occurring in greater than 80% of cases during the third trimester.[39]
The diagnosis of Lassa fever can be made by Enzyme-Linked Immunosorbent Assay (ELISA), Immuno-fluorescence test (IT), Real-time Polymerase Chain Reaction (RT-PCR), Virus isolation by cell culture, and post-mortem diagnosis, by immuno-histochemistry on tissue.[40] Early diagnosis and isolation are crucial for enhancing survival and reducing transmission.
The mainstay of treatment is early recognition of infection coupled with effective isolation, early initiation of the antiviral drug ribavirin, and the best available supportive care in a hospital setting.[41] The treatment of Lassa fever should be at an isolation facility to limit the potential for nosocomial infection. Health workers should have a high index of suspicion for all febrile illnesses in endemic areas that do not respond to initial treatment, screen for Lassa fever, and institute standard precaution measures, such as masks, boots, goggles, aprons, and gloves.[42] The drug of choice is parenteral Ribavirin, which is most effective when started early, with supportive treatment as indicated and recommended by the clinician. Intravenous Ribavirin has been shown to reduce mortality from 55% to 5% if administered within the first 6 days of illness.[43] The clinician should manage pain and fever with a simple analgesic/antipyretic such as paracetamol. Clinicians or health workers should avoid the use of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) in suspected cases of Lassa fever because of bleeding-related complications. Diarrhea occurs in 50% of cases; patients with significant diarrhea should have regular assessment of their electrolytes, with replacement provided as necessary. Intravenous fluids should be initiated and titrated to maintain adequate volume status in patients requiring hospital admission.[44]
People who have traveled with, lived with, or cared for an individual with Lassa fever within the past 21 days and who are asymptomatic should be traced, assessed, and provided with post-exposure prophylaxis with Ribavirin.[45]
2.3. Healthcare Workers (HCWs)
Healthcare workers (HCWS) are critical in running fit-for-purpose infection prevention and control measures in a hospital setting. The knowledge, attitude, and practice of the HCWs regarding IPC measures set the pace for the successful introduction, implementation, and enforcement of IPC measures. HCWs provide leadership, and their attitude and behavior can positively or negatively influence the attitude and behavior of patients, their caregivers, and the hospital community regarding IPC measures. HCWs should be knowledgeable about infectious agents, their mode of transmission, symptoms, and the standard precaution measures for prevention and control.[46] [47] [48]
The HCWs play vital roles in setting the protocol, defining roles and responsibilities, and implementing and enforcing the IPC rules and regulations towards achieving the overarching aims and objectives of promoting patients’ well-being and quicker recovery and reducing the risk of hospital-acquired infection. The HCWs, ranging from doctors, nurses, pharmacists, laboratory scientists, record clerks, attendants, and cleaners, play different but complementary roles and are invaluable in smoothly operationalizing the hospital IPC measures. [49] [50] [51]
2.4. Knowledge, Attitudes and Practices (KAP)
The proper knowledge, attitude, and practice are critical in implementing and enforcing IPC measures. The KAP model illustrates the importance of KAP in implementing IPC measures. The HCWs can only give what they have, so acquiring optimal knowledge through training and re-training is necessary for building the right attitude and disposition to practice and adhere to standard precautions and IPC measures. Knowledge usually predicts attitude, and attitude greatly influences acceptance, practice, and adherence to IPC measures.[52]
Lassa fever is predominantly transmitted in hospital settings through contact with infected individuals or their body fluids, and standard precautions are crucial in preventing hospital-acquired infections. HCWs are at the center of patients’ care and treatment. They are at significant risk of contracting Lassa fever from one patient and passing it to other patients if they do not practice standard precautions and always adhere to the hospital IPC protocol.[53] [54] The key to stopping hospital-acquired Lassa fever outbreaks or sustained transmission in a hospital setting is for the HCWs to have a high index of suspicion of infectious diseases, including Lassa fever and other viral hemorrhagic fevers, like Ebola, Marburg, and so forth. Frontline healthcare workers, working in the Accident and Emergency ward or caring for very sick patients, must be knowledgeable about these diseases, their seasonal patterns, and presentations. They should be on the lookout for them, especially during seasonal outbreaks in neighboring towns, cities, or districts.[55]
- Methodology
These interrelationships between the variables required both quantitative and qualitative approaches in answering the research questions.
3.1. Research Design
A sequential explanatory mixed-methods design was utilized to understand their awareness, knowledge, attitudes, and practices regarding Lassa fever prevention and control measures. The study tools involved structured questionnaires, key informant interviews (KII), and focus group discussions (FGD). It employed both empirical and qualitative approaches, described, explored, and investigated the phenomenon in-depth, and provided a comprehensive understanding of the subject matter. This approach was suitable for health behavior research as it allowed the emergence of themes and patterns grounded in real-world experiences of healthcare workers.
3.2. Study Setting
The study was conducted in Barau Dikko Teaching Hospital (BDTH), Kaduna State, Nigeria. BDTH, a tertiary facility owned by the state government and a teaching hospital for Kaduna State University, was purposefully sampled for the research. It is centrally located and serves as an isolation, diagnosis, and treatment center for Lassa fever cases, catering to the 23 Local Government Areas (LGAs) of Kaduna State.[56] [57]
3.3. Study Population
Health workers (including doctors, nurses, pharmacists, lab technicians and technologists, record keepers and other clinical staff) were randomly sampled from the 14 clinical Departments (namely Accident & Emergencies, Surgery, Radiology, Physiotherapy, Pharmacy, Pathology, Ophthalmology, Medical Microbiology, Hematology, Dental, Gynecology, Pediatrics, Medicine, and the Tuberculosis Clinic) at Barau Dikko Teaching Hospital (BDTH), Kaduna participated in the research.
3.4. Sampling Technique
Participants were randomly sampled from a list of clinical staff maintained at 14 clinical departments of BDTH to complete the research questionnaires. Randomly sampled health workers, especially those representing a cross-section of departments and professional roles, were further selected for in-depth interviews. A total of 15 respondents who completed the survey participated in the key informant interviews, and one (1) focused group discussion was conducted with the heads of different departments or representatives.
3.5. Sample Size Estimation
The sample size was estimated using a formula (Cochran’s), factoring the prevalence of good knowledge of Lassa fever in Kaduna State, at 5% significance level and 80% power. To account for potential non-response, attrition, or incomplete questionnaires, a 10% oversampling rate was applied.[58]
3.6. Sample Size Distribution
The Probability Proportional to Size (PPS) technique was employed to ensure a fair and representative allocation of the total sample size across the 14 clinical departments of Barau Dikko Teaching Hospital (BDTH). Under this approach, the number of participants selected from each department was proportional to the total number of clinical staff within that department. This method enhanced representativeness, reduced sampling bias, and ensured that departments with larger staff sizes contributed a greater number of respondents to the study than those with smaller staff sizes. It also allowed for meaningful comparisons between departments in terms of knowledge, attitudes, and practices regarding Lassa fever infection prevention and control.
3.7. Methods of Data Collection
Questionnaires were administered with the aid of electronic devices using the Open Data Kit (ODK) platform, to the randomly sampled health workers, while FGD and key informants’ interviews were conducted for qualitative data collection. The Human-Centered Design (HCD) framework was employed for both quantitative and qualitative data collection. Field notes and audio recordings complemented the interviews, enriching qualitative insights and ensuring contextual accuracy.
3.8. Definition & Measurement of Variables
Awareness: Awareness of Lassa fever was assessed using a 5-point categorical question. Each correct response to the categorical question was scored 1 mark. A cumulative score of less than 2 was assessed as poor awareness, 2–3 as fair awareness, and a score of 4 or higher as good awareness.
Knowledge: Knowledge of Lassa fever was assessed using a 20-point scoring system based on basic knowledge of the etiology, disease vector, mode of transmission, clinical features, drug treatment, and preventive measures against Lassa fever. This section comprises 5-item, and each correct response was scored 1 mark. A score of less than 10 was assessed as poor knowledge; 10-15 was considered fair knowledge, while a score of ≥16 was assessed as good knowledge.
Attitude: Attitude was assessed using a 6-point scoring system comprising graded responses to specific preventive measures on a 5-point Likert scale and categorical questions. The responses to the 4-item questionnaire were graded as follows: 2.5 = very positive/very confident, 2.0 = positive/confident, 1.5 = Neutral, 1.0 = negative/not confident, and 0.5 = very negative/not confident at all. Each correct response to the categorical question was scored 1 mark. A cumulative score of less than 2 was assessed as a poor attitude; 2 – 4 as a fair attitude, and a score of ≥5 was assessed as a good attitude.
Practices: The practices of IPC measures among healthcare workers who participated in the study were assessed and graded using an 8.5-point scoring system. The responses to the 4-item questionnaire were graded as follows: 2.5 = always, 2.0 = frequently, 1.5 = sometimes, 1.0 = rarely, and 0.5 = never. Each correct response to the categorical question was scored 1 mark. A score of less than 3 was graded as poor IPC practice; 3 – 5 as fair IPC practice, and 6 and above was graded as good IPC practice.
Local Realities and Global Implications: The local realities and global implications of the health workers’ knowledge, attitudes, and practices regarding Lassa fever IPC were assessed and graded using a 9-point scoring system. The responses to the 3-item questionnaire were graded as follows: 2.5 = very well prepared/strongly agree, 2.0 = prepared/agree, 1.5 = neutral, 1.0 = unprepared/disagree, and 0.5 = very unprepared/strongly disagree. Each correct response for the categorical question scored 1 mark, and the total score was interpreted to reflect levels of preparedness and awareness relevant to global and local disease prevention and control measures.
The composite scores were adapted from prior work on KAP of healthcare workers regarding Lassa fever IPC measures in a clinical setting in Edo State, Nigeria.[59]
3.9. Validity and Reliability of Research Instrument
The study tool has demonstrated good content validity and dependable test-retest reliability, as shown in previous studies on the knowledge, attitudes, and practices of health workers regarding Infection Prevention and Control in healthcare facility settings.[60] The content validity was established through a rigorous and iterative review process that incorporated expert opinions from epidemiologists, public health professionals, and infectious disease specialists. This practice ensured that the instrument adequately captured all relevant aspects of knowledge, attitude, and practices (KAP) related to Lassa Fever IPC measures.
The study tool was pre-tested (in a pilot study) among a small subset of healthcare workers, and the results were analyzed for internal consistency using Cronbach’s alpha coefficient (α = 0.75). The tool demonstrated a high level of reliability, indicating its consistency in measuring the intended variables over time. Additionally, the test-retest method was applied, where the same participants were reassessed after a two-week interval. The findings showed minimal intra-participant variation, reinforcing the instrument’s stability and reliability.
Moreover, the tool underwent face, content, and construct validity assessments, where respondents were asked to provide feedback on question clarity, language simplicity, structural flow, comprehensiveness, and relevance. Their input was incorporated to refine ambiguous questions and ensure that the target population easily and accurately understood the terminology. The researcher optimized the study tool’s accuracy, consistency, and applicability across diverse healthcare settings by integrating qualitative and quantitative validation techniques. Data from various sources, both qualitative and quantitative, were triangulated to ensure the accuracy, consistency, and validity of the data. The researcher reviewed all the data, corrected significant missing data, and contacted some respondents to clarify observed errors, which ultimately guaranteed data accuracy and appropriateness.
3.10. Research Procedure
Before recruiting participants, ethical approval was obtained from the Health Research and Ethical Committee (HREC) of BDTH Kaduna. The research proceeded in the following order: a questionnaire-based survey, Key Informant Interview (KII), and Focus Group Discussion (FGD). The participants who completed the research questionnaire were contacted, and suitable dates were agreed upon for the key informant interview (KII) and the FGD sessions. The FGD and KII lasted about 1 hour, with all sessions recorded and transcribed. Before data collection, research assistants were trained on the study protocol, ethical considerations, and use of data collection tools to ensure uniformity and quality.
3.11. Inclusion & Exclusion Criteria
All clinical staff employed for 1 year or more, randomly sampled, working in BDTH Kaduna, and who voluntarily provided informed consent, participated in the study.
Students in training and interns, health workers in isolation centers, and health workers on temporary employment were excluded from the study.
3.12. Data Analysis
The researcher used the Statistical Package for Social Sciences (SPSS) in data collation. Descriptive statistics for proportions and measures of central tendency were calculated. The researcher conducted a Chi-square test to determine associations between categorical variables. Pearson’s correlation coefficient was utilized to assess the relationship between the variables. Records of FGD and interviews were cleaned for consistency, transcribed, and analyzed for emerging themes. The themes were coded based on identified patterns that addressed the research questions.[61]
3.13. Ethical Considerations
Before fieldwork, ethical approval (NHREC/BDKHREC/27/238) was obtained from the BDTH, Kaduna State, Health Research and Ethical Committee (HREC). The data was anonymized, and no information can be traced back to any individual. Only respondents who willingly gave written informed consent after a clear explanation of the protocol by the researcher participated in the study.
Participants were informed of their right to withdraw at any time without any consequences. The researcher maintained the privacy and confidentiality of respondents’ information throughout the research, and data was encrypted and stored electronically in an anonymized form. All data was stored securely, and access was restricted to the research team only. Confidentiality, voluntary participation, and the principle of ‘do no harm’ guided all aspects of the research.
- Findings and Discussion
The paper explored the dynamics of infectious diseases and the knowledge, attitudes and practices of healthcare workers at BDTH regarding Lassa Fever IPC measures.
4.1. General Characteristics of the Respondents
A total of 398 healthcare workers were sampled for the study; 388 (97%) consented, while 10 (3%) withheld consent to participate. The data were cleaned, and 3 (0.8%) respondents were discarded due to significant missing data, leaving 385 (99.2%) respondents for analysis. The mean age of the respondents was 41 years, with a standard deviation (SD) of 10, and a range of 20 to 67 years (Table 1). The sex distribution of the respondents was as follows: female, 258 (67%); and male, 127 (33%). A higher proportion of the respondents, 183 (48%), were nurses, followed by doctors 70 (18%), laboratory technicians 40 (10%), public health officers 28 (7%), and others (pharmacists, medical health record officers, nutritionists, dental technicians, physiotherapists, radiographers) 64 (17%).
The data analysis revealed that 138 (36%) of the respondents had 16 years or more experience in the health sector, 104 (27%) had 6 to 10 years, 75 (19%) had 0 to 5 years, and 68 (18%) had 11 to 15 years of experience. At the highest level of education attained, 232 (60%) of the respondents held tertiary education, 138 (36%) had postgraduate education, and 14 (4%) had fellowship qualifications. It is worth stating that only one respondent had a secondary education. The data analysis revealed that 98% of the respondents provided services at the teaching hospital, while 2% provided services at the specialist hospital.
Table 1: Demographic Characteristics of the Respondents
| Characteristics (n=385) Frequency Percentage (%) |
| Age (Years)
18-25 18 5 26-35 121 31 36-45 138 35 46-60 106 28 60 and Above 2 1 M±SD 41±10 Gender Female 258 67 Male 127 33
Job Title/Position Doctor 70 18 Laboratory Technician 40 10 Nurse 183 48 Public Health Officer 28 7 Others1 64 17
Years of Experience in the Health Sector 0-5 75 19 6-10 104 27 11-15 68 18 16 and Above 138 36
Highest Level of Education Attained Secondary 1 <1 Tertiary (Undergraduate) 232 60 Post-graduate 138 36 Others2 14 4
Type of Healthcare Facility You Work at Specialist Hospital 7 2 Teaching Hospital 378 98
|
1Pharmacists, Medical Health Record Officers, Nutritionists, Dental Technicians, Physiotherapists, Radiographers; 2Fellowship Qualification; M=Mean; SD=Standard Deviation
4.2. Awareness of Lassa Fever among Respondents
A total of 384 (99.7%) of the respondents were aware of Lassa fever as a public health concern in Nigeria (Table 2). On formal training, seminar, or briefing on Lassa fever and its prevention in the past 12 months, 124 (32%) of the respondents had received formal training, 57 (67%) had no formal training, and 4 (1%) of the respondents were not sure of their status on formal training, seminar, or briefing on Lassa fever. Regarding Lassa fever transmission, 383 (99%) respondents were aware that the disease can be transmitted through contact with food or items contaminated by rodent urine or feces. Only 2 (1%) respondents were unaware that Lassa fever can be transmitted through contact with food or items contaminated by rodent urine or feces.
On infection prevention and control (IPC) guidelines specific to Lassa fever at BDTH, 312 (81%) of the respondents were familiar with the infection prevention and control (IPC) guidelines specific to Lassa fever in Barau Dikko Teaching Hospital (BDTH), Kaduna. In comparison, 47 (12%) were not familiar, and 2 (7%) were indecisive (not sure) of their familiarity with the IPC guideline.
On awareness campaign or distribution educational materials, 174 (45%) of the respondents were aware BDTH conducted awareness campaign or distributed educational materials (e.g., posters, leaflets, handbooks) on Lassa fever in the past year, 151 (39%) were not ware, and 60 (16%) respondents were not sure of any awareness campaign or distribution of educational materials on Lassa fever in the past year, at BDTH.
Table 2: Respondents’ Awareness of Lassa Fever and IPC Measures
| Characteristics (n=385) Yes No Not Sure
Freq. (%) Freq. (%) Freq. (%) |
| Are you aware of Lassa fever? 384 (99.7%) 1 (0.3%) 0 (0%)
Have you received any formal training? 124 (32%) 257 (67%) 4 (1%) Aware of Lassa fever transmission? 383 (99%) 2 (1%) 0 (0%) Familiar with Lassa fever IPC measures? 312 (81%) 47 (12%) 26 (7%) HF conducted any awareness campaign? 174 (45%) 151 (39%) 60 (16%) |
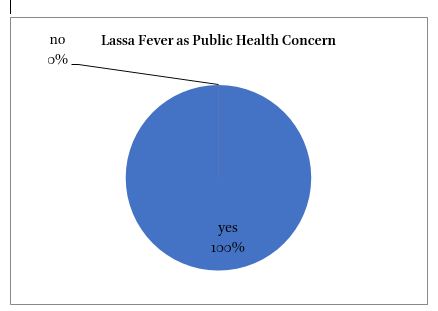
Figure 2: Awareness of Lassa Fever as a Public Health Concern in Nigeria among Respondents
4.3. Knowledge of Lassa Fever among Respondents
On dynamics of infectious diseases, especially Lassa fever, 310 (80%) of the respondents were familiar with the dynamics of infectious diseases, especially Lassa fever, 60 (16%) were neither familiar nor not familiar, and 15 (4%) were not familiar with the dynamics of infectious diseases, Lassa fever (Table 3). On the contributory factors to the recurrent Lassa fever outbreaks in Kaduna State, 369, 96% (hand hygiene); 356, 92% (rodent exposure); 347, 90% (awareness of Lassa fever); 309, 82% (inadequate infrastructure); 316, 82% (poor community health practices) of the respondents believed these five factors contributed to the recurrent Lassa fever outbreaks in Kaduna State.
About 13 (3%) respondents identified poverty, poor government commitment, bush burning, insufficient budget by the government, and non-adherence to IPC protocol, were also listed by 13 (3%) respondents, as contributory factors to the recurrent Lassa fever outbreaks in Kaduna State. On symptoms of Lassa fever, 378, 98% (fever); 340, 88% (headache); 289, 75% (vomiting); 241, 63% (abdominal pain); 208, 54% (cough); 265, 69% (diarrhea); 328, 85% (fatigue); and 355, 92% (bleeding) of the respondents agreed these eight symptoms were manifestations of Lassa fever. Other symptoms, such as sore throat, rashes, jaundice, and body weakness, were also mentioned by 23 (6%) respondents as symptoms of Lassa fever.
The majority of respondents, 261 (67%), agreed that rodent exposure was the primary mode of Lassa fever transmission, 118 (31%) reported contact with bodily fluids, and 6 (2%) indicated airborne transmission. On Lassa fever infection prevention and control (IPC) measures, 330, 86% (safe handling of body fluids); 264, 69% (rodent control measures); 327, 85% (use of PPEs); 347, 90% (isolation of suspected cases); and 346, 90% (regular hand washing) of the respondents agreed these five-infection prevention and control (IPC) measures were in place in BDTH for Lassa fever prevention and control. Other IPC measures, including contact tracing, an effective surveillance system, post-exposure prophylaxis, proper waste disposal, a hotline for suspected cases, and Information, Education, and Communication Materials (IEC), were also listed by 11 (3%) respondents as available IPC measures in BDTH for Lassa fever prevention and control.
Table 3: Respondents’ Knowledge of Lassa Fever
| Characteristics (n=385) Frequency Percentage |
| Familiar with the dynamics of infectious disease?
Familiar 310 80 Neither familiar or not familiar 60 16 Not familiar 15 4 What are the contributing factors to the LF outbreak? Poor hygiene & Sanitation 369 96 Rodent Exposure 356 92 Lack of awareness about LF 347 90 Inadequate healthcare infrastructure 309 80 Poor community health practices 316 82 Others1 13 3 Which of the following are symptoms of LF? Fever 378 98 Headache 340 88 Vomiting 289 75 Abdominal pain 241 63 Cough 208 54 Diarrhea 265 69 Fatigue 328 85 Bleeding 355 85 Others2 23 6 What is the primary mode of LF transmission? Airborne 6 2 Contact with bodily fluids 118 31 Rodent exposure 261 67 What LF IPC measures are in place in your HF? Safe handling of bodily fluids 330 86 Rodent control measures 264 69 PPEs use 327 85 Isolation of suspected cases 347 90 Regular hand washing 346 90 Others3 11 3 |
1Poverty, poor government commitment, bush burning, insufficient budget by government, non-adherence to IPC protocol; 2Sore throat, rashes, jaundice, body weakness; 3Contact tracing, effective surveillance system, post-exposure prophylaxis, proper waste disposal, hotline for suspected cases, Information Education and Communication Materials (IEC)
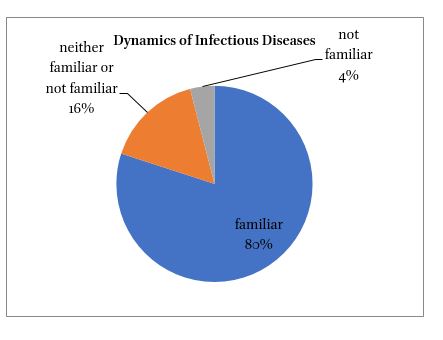
Figure 3: Distribution of Respondents’ Familiarity with the Dynamics of Infectious Diseases, especially Lassa Fever
4.4. Attitudes to Lassa Fever among Respondents
On attitude toward the IPC measures for Lassa fever, 137 (35%) of the respondents had a very positive attitude, 199 (52%) positive attitude, 7 (2%) had a negative attitude, and 42 (11%) had neither positive nor negative attitude (neutral) toward Lassa fever IPC measures (Table 4). On confidence in your ability to manage and prevent Lassa fever infections at BDTH, 99 (26%) were very confident, 197 (51%) were confident, 24 (6%) were not confident, and 24 (6%) of the respondents were ambivalent (neutral) about confidence in their ability to manage and prevent Lassa fever at BDTH. Only 1 (<1%) respondent was not confident at all in the ability to manage and prevent Lassa fever at BDTH. Most of the respondents, 354 (92%), agreed (yes) that IPC measures effectively reduced the spread of Lassa fever in BDTH. In comparison, 12 (3%) disagreed (no), and 19 (5%) were indecisive (not sure) on the effectiveness of IPC measures in Lassa fever control at BDTH.
Table 4: Respondents’ Attitudes towards Lassa Fever
| Characteristics (n=385) Frequency Percentage |
| What is your attitude towards LF IPC measures?
Very positive 137 35 Positive 199 52 Neutral 42 11 Negative 7 2 Very negative 0 0 How confident are you to manage and prevent LF? Very confident 99 26 Confident 197 51 Neutral 64 17 Not confident 24 6 Not confident at all 1 <1 Do you believe in the effectiveness of LF IPC measures? No 12 3 Not sure 19 5 Yes 354 92
|
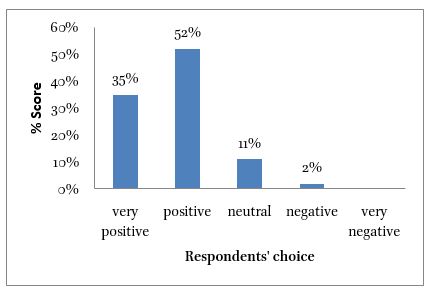
Figure 4: Distribution of Respondents’ Attitudes toward the IPC Measures for Lassa Fever
4.5. Infection Control and Prevention Practices among Respondents
On practice of hand hygiene (hand-washing or using alcohol-based hand rub) when dealing with patients suspected of having Lassa fever, 246 (63%) of the respondents practiced hand hygiene always, 110 (29%) frequently, 26 (7%) sometimes, 2 (1%) rarely and 1 (<1%) never (Table 5). On the use of personal protective equipment (PPE) when attending to suspected or confirmed Lassa fever cases, 231 (60%) of the respondents used PPE always, 95 (25%) frequently, 47 (12%) sometimes, 7 (2%) rarely, and 5 (1%) never.
On adherence to the recommended IPC protocols (e.g., isolation of suspected cases, decontamination of surfaces) at BDTH, 236 (61%) of the respondents followed the recommended IPC protocol always, 103 (27%) frequently, 40 (10%) sometimes, 5 (1%) rarely, and 1 (<1%) never. The majority of the respondents, 204 (53%), agreed (yes) that the IPC measures in place at BDTH were sufficient to control Lassa fever outbreaks, 129 (33%) disagreed (no), and 52 (14%) were indecisive (not sure) on the sufficiency of the IPC measures at BDTH to control Lassa fever outbreaks.
Table 5: Respondents’ Practices Regarding Lassa Fever
| Characteristics (n=385) Frequency Percentage (%) |
| How frequently do you practice hand hygiene in response to LF?
Always 246 63 Frequently 110 29 Sometimes 26 7 Rarely 2 1 Never 1 <1 Do you use PPEs in response to LF? Always 231 60 Frequently 95 25 Sometimes 47 12 Rarely 7 2 Never 5 1 Do you follow the recommended IPC protocols in your HF? Always 236 61 Frequently 103 27 Sometimes 40 10 Rarely 5 1 Never 1 <1 Do you feel the IPC measures are sufficient to control the LF outbreak? Yes 204 53 No 129 33 Not sure 52 14 |
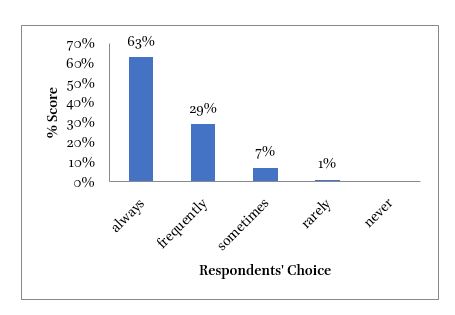
Figure 5: Distribution of Respondents Practice Hand Hygiene (Handwashing or Using Alcohol-based Hand Rub) when Dealing with Patients Suspected of Having Lassa Fever
4.6. Perception of Lassa Fever Local Realities and Global Cooperation among Respondents
On how prepared was Kaduna State health system to manage recurrent Lassa fever outbreaks, 41 (11%) of the respondents agreed the local health system was very well prepared, 183 (48%) prepared, 48 (12%) unprepared, 8 (2%) very unprepared, and 105 (27%) ambivalent (neutral) on the preparedness of the Kaduna State health system to manage recurrent Lassa fever outbreaks (Table 6).
On the subject of global cooperation and knowledge sharing in managing Lassa fever more effectively, 235 (62%) of the respondents strongly agreed, 148 (38%) agreed, 1 (<1%) disagreed, and 1 (<1%) was ambivalent (neutral) about the role of global cooperation and knowledge sharing in managing Lassa fever outbreaks more effectively in Kaduna State. On additional measures to improve prevention and control of Lassa fever in Kaduna State, 377, 98% (increased community awareness campaigns), 374, 97% (more training for healthcare workers), 349, 91% (enhanced diagnostic tools and equipment), and 354, 92% (stronger inter-facility coordination) of the respondents agreed on the relevance of these four measures in strengthening Lassa fever IPC measures in Kaduna State. Other measures, application of accountability measures, behavior change campaign, better funding of IPC measures, effective rodent control measures, free treatment for Lassa fever cases, functional hospital IPC committee, better staffing of the hospital, improved environmental sanitation, were among the measures suggested by 25 (6%) of the respondents to improve Lassa fever IPC in Kaduna State.
Table 6: Respondents’ Perception of Local Realities and Global Implications
| Characteristics (n=385) Frequency Percentage (%) |
| How prepared is your local health system to manage LF outbreak?
Very well prepared 41 11 Well prepared 183 48 Neutral 105 27 Unprepared 48 12 Very unprepared 8 2
Do you think global cooperation could help in managing LF outbreak? Strongly agree 235 62 Agree 148 38 Neutral 1 <1 Disagree 1 <1 Strongly disagree 0 0
What additional measures should be taken in Kaduna State to improve LF response? Increased community awareness campaigns 377 98 More training for healthcare workers 374 97 Enhanced diagnostic tools and equipment 349 91 Stronger inter-facility coordination 354 92 Others1
|
1Application of accountability measures, behavior change campaign, better funding of IPC measures, effective rodent control measures, free treatment for Lassa fever cases, functional hospital IPC committee, better staffing of the hospital, improved environmental sanitation
Figure 6: Distribution of Respondents on Preparedness of Kaduna State Health System to Manage Recurrent Lassa Fever Outbreaks
Figure 7: The Respondents Category on Awareness, Knowledge, Attitudes, Practice, and Local Realities and Global Implications on Lassa Fever IPC at BDTH, Kaduna
4.7. g) Analysis of Reported Lassa Fever in Kaduna State, 2019-2024
Desk review of surveillance data, extracted from Surveillance Outbreaks Reporting Management and Analysis System (SORMAS) in Kaduna State, showed 50 persons lost their lives to Lassa fever, between 2019 and 2024, from 564 reported Lassa Fever cases, 520 suspected, and 44 confirmed (Table 7).
Table 7: Analysis of Reported Lassa Fever in Kaduna State, 2019-20241
| Year Reported Case Admission Outcome
Susp Confirmed Adm not Adm Death Recovered |
| 2019 52 4 5 51 1 55
2020 159 9 10 158 4 164
2021 52 0 5 47 2 50
2022 117 12 17 112 18 111
2023 46 2 12 36 8 40
2024 94 17 7 104 17 94
Total 520 44 56 508 50 514 |
1Source: Kaduna State Ministry of Health, Epidemiological Diseases Division, Extracted from the Surveillance Outbreaks Reporting Management and Analysis System (SORMAS) data.
4.8. Association between Awareness, Knowledge, Attitudes, and Practices, and the Perception of Local Realities and Global Implications of Lassa Fever
There was no statistically significant difference in respondents’ awareness of Lassa fever IPC measures based on the job title or position and years of experience in the health sector, χ2=4.88, P=0.77, and χ2=8.26, P=0.22, respectively. There was no statistically significant difference in respondents’ knowledge of Lassa fever IPC measures based on job title or position, and years of experience in the health sector, χ2 = 6.23, P = 0.62, and χ2 = 2.35, P = 0.88, respectively. There was a statistically significant difference in respondents’ attitudes towards Lassa fever IPC measures based on job title or position, χ2 = 20.95, P = 0.007. However, there was no statistically significant difference in respondents’ attitudes based on the years of experience in the health sector, χ² = 7.86, p = 0.247. There was no statistically significant difference in respondents’ practices regarding Lassa fever IPC measures based on job title or position, and years of experience in the health sector, χ2 = 1.46, P = 0.96, and χ2 = 3.01, P = 0.81, respectively. There was no statistically significant difference in respondents’ perception of the local realities and global implications of Lassa fever IPC measures based on job title or position and years of experience in the health sector, χ2 = 1.16, P = 0.99, and χ2 = 4.06, P = 0.69, respectively.
A strong positive relationship was found between health workers’ overall scores on awareness, knowledge, attitudes, practice, and perception of local realities and global cooperation, based on job title or position and years of experience in the health sector, with a correlation coefficient of r = -0.999.
4.9. Thematic Analyses
Eleven (11) thematic areas, roles and responsibility, understanding of infection causes, perception of Lassa fever outbreaks, drivers or causes of Lassa fever outbreaks, disease occurrence and environmental impact, impact of ecosystem changes, awareness of BDTH IPC measures, effectiveness of BDTH IPC measures, training on IPC measures, challenges in IPC practice, and solutions to overcoming challenges were identified after transcription, coding, and analyses of respondents’ views, opinions and recommendation during the KII and FGD.
In summary, the healthcare workers demonstrated a good understanding of the Dynamics of Infectious Diseases and the interrelatedness of disease, host, environment, climate, and biodiversity in the occurrence, transmission, and response to infectious diseases, such as Lassa Fever, within a rapidly evolving ecosystem.
4.10. Relevance & Relationship with Similar Studies
The study, employing both qualitative and quantitative approaches, demonstrated that healthcare workers at Barau Dikko Teaching Hospital (BDTH), Kaduna, possessed a sound understanding of the dynamics of infectious diseases and the impact of recurrent Lassa Fever outbreaks in Kaduna State, Nigeria. They were also aware of the factors driving persistent outbreaks, as well as the importance and relevance of Infection Prevention and Control (IPC) measures in controlling and preventing Lassa Fever outbreaks at BDTH, Kaduna, and in the surrounding community.
The study revealed that healthcare workers at BDTH, Kaduna, had above-average performance scores in awareness (71%), knowledge (81%), attitudes (85%), practices (79%), and local and global implications (89%) regarding Lassa Fever IPC measures. The healthcare workers demonstrated a robust understanding of the ecosystem and the interrelatedness of disease, host, environment, climate, and biodiversity in the occurrence, transmission, and response to infectious diseases, such as Lassa Fever.
These findings were consistent with the results from previous empirical studies on healthcare workers’ knowledge, attitudes, and practices regarding Lassa fever IPC measures in tertiary facilities in Abakiliki and Owo, Nigeria, as well as a qualitative study in Freetown, Sierra Leone.[62] [63] [64] [65] The findings also showed that healthcare workers in tertiary facilities had higher scores in knowledge, attitudes, and practices compared to colleagues in primary and secondary facilities.[66]
The study revealed that only attitudes showed a statistically significant association with respondents’ scores on Lassa Fever IPC measures based on the job titles or position and years of experience in the health sector. However, awareness, knowledge, and practices showed no statistically significant association in respondents’ scores on Lassa Fever IPC measures based on the job title or position and years of experience in the health sector. The study also showed a strong positive correlation between respondents’ years of experience in the health sector and job title or position.
4.11. Implications
The study has revealed that about 50 people lost their lives to Lassa Fever in Kaduna State between 2019 and 2024, as shown in the desk review of surveillance records from the Kaduna State Ministry of Health, Epidemiological Division (Table 7).
The study has shown that Lassa Fever remains a critical public health concern, and IPC measures are essential in interrupting Lassa fever transmission and the attendant mortality and morbidity. It also demonstrated that healthcare workers were key in Lassa fever IPC measures implementation, and effective practice of Lassa Fever IPC measures depended on healthcare workers’ optimal knowledge, positive attitudes, availability of PPE, and facilities for hygiene and sanitation, enforcement of Lassa Fever IPC measures, and involvement of the community and development partners.
The study has revealed that the attitudes of healthcare workers can predict behavior, adherence, and the practice of IPC measures in both hospital settings and communities, serving as a reliable entry point for IPC policy reform, implementation, and enforcement.
Moreover, it has provided empirical and qualitative evidence that recurrent Lassa Fever outbreaks in Kaduna State are driven by non-adherence to standard precautions and Lassa Fever IPC guidelines in hospital settings and communities. In addition, the insufficiencies in IPC facilities were worsened by suboptimal knowledge of IPC measures, negative attitudes among healthcare workers, and inadequate enforcement of accountability measures by hospital management.
The study findings are expected to have a positive impact on IPC policy reforms, healthcare workers’ capacity development, strengthening of the IPC system, and improvements in overall public health outcomes in Kaduna State.[67] [68] [69]
4.12. Recommendations
The following recommendations will address the identified challenges, facilitate effective implementation of Lassa fever IPC measures, and guarantee safety and protection for healthcare workers and their clients. The tasks are immense, and addressing the identified challenges, providing the necessary facilities and commodities, and having a well-trained and motivated staff are collaborative efforts between hospital management, health authorities, and development partners.
- Personal Protective Equipment (PPE)
The availability of PPE (gloves, facemasks, gowns, boots, goggles) in the correct quantity, quality, and sizes in clinics, theatres, departments, and wards will shore up healthcare workers’ confidence in standard precaution and IPC measures during procedures, laboratory tests, operations, and handling of potentially hazardous specimens. The availability of PPE is critical to the practice of Lassa fever IPC, and maintaining a constant supply through robust logistics plans will go a long way in reducing stockouts and ensuring healthcare workers do not take unnecessary risks while caring for patients. During the interviews and discussions, the respondents clearly underscored the importance of PPE in practicing Lassa Fever IPC measures.
“No. PPEs are not readily available. We need more PPE to protect ourselves while responding to infectious diseases like Lassa Fever.”
b) Staff Training
There is a need for regular staff training, primarily newly recruited staff, on Lassa Fever IPC. The training should be hands-on, incorporating practical demonstrations and simulations to reinforce key messages and enhance healthcare workers’ knowledge, attitudes, and practices regarding Lassa Fever IPC measures at BDTH, Kaduna. Training needs became clear from the respondents during the interviews and discussions as one of the critical requirements for effective Lassa fever IPC.
“Not regular. The training is not routine, but reactive during outbreaks. We need regular training to better practice Lassa fever IPC measures.”
c) Staff Motivation and Recruitment
Staff motivation and recruiting adequate staff in the correct numbers and expertise will promote better Lassa Fever IPC practice, on-the-job mentorship for young colleagues, and positive reinforcement of good behaviors and practices. A well-motivated staff can adapt to changes and deliver on set goals. During the interviews and discussions, the respondents underscored the importance of staff welfare, better working conditions, and motivation.
“Better staffing and improved remuneration and staff motivation will contribute to better practice of Lassa Fever IPC measures.”
- Water, Sanitation, and Hygiene Facilities
The regular supply of water, essential commodities for sanitation such as soap, detergents, and disinfectants, as well as the availability of washing equipment, were critical for maintaining hand hygiene and keeping the hospital free of microorganisms. The availability of water and sanitation facilities, tools, and equipment for hand hygiene and sanitation was at the top of respondents’ requirements for effective Lassa Fever IPC.
“Facilities for sanitation, water, soap, and other supplies are not freely available, as and when needed in response to Lassa fever and other infectious diseases. We need a regular water supply, hand hygiene, and sanitation commodities.”
- Rodent Control Measures
Rodent control measures were another key requirement for effective Lassa Fever IPC, as rats and other rodents freely move through the facility, especially at night. It will reduce staff and patient exposure to rats and Lassa fever infection, as well as their transmission within the hospital community.
“Need for rodent control measures. It will reduce the risk of Lassa fever outbreaks.”
- IPC Policy and Committee Engagement
The hospital IPC committee should meet regularly and recommend policy changes and strategies to effectively implement Lassa fever IPC measures. Healthcare workers and hospital management should prioritize the availability and visibility of IPC policies and their implementation. Efforts should be made to update them and increase their visibility to staff, clients, and caregivers.
“Yes. The IPC measures are more reactive and are not adequately displayed in strategic places for public consumption. IPC measures should be regularly revised and communicated to staff.”
- Funding and Resource Allocation
More funding allocation to IPC measures will provide the basic facilities, PPE, equipment, and commodities needed for effective Lassa Fever IPC. The intervention of government and development partners will be critical in augmenting the meager funds allocated to Lassa Fever IPC measures at BDTH, Kaduna, given the hospital’s tight budget and inadequate revenue to meet demands for effective Lassa fever IPC.
“Better funding for IPC measures will contribute to the effective implementation of IPC measures.”
- Government and Development Partner Engagement
There is a need for improved government involvement and engagement of development partners in providing needed PPE, equipment, facilities, technical support, and leadership in the design, implementation, and evaluation of Lassa fever IPC measures at BDTH, Kaduna. In addition to providing catalytic funding for critical programs and interventions in Lassa Fever IPC, government, Non-governmental Organizations, and development partners, like WHO, UNICEF, and others, should provide technical support and policy direction on Lassa Fever IPC measures, and overarching leadership on environmental sanitation and implementation of one health approach policy in the control and prevention of emerging and re-emerging diseases.
“Stronger engagement with the hospital management for more funds to IPC measures.”
- Community Involvement
There is a need for greater community involvement in rodent control, the use of rodent-proof containers for storing grains, avoiding the drying of grains on roads and bare floors, enforcing a ban on bush burning, promoting a clean environment and proper refuse disposal, and educating the public on hand and personal hygiene. Community involvement was another critical requirement for effective and comprehensive Lassa fever IPC in BDTH and the immediate community.
“Practicing better food processing and storage methods, personal hygiene and environmental sanitation, and improved awareness of Lassa fever infection through education and sensitization.”
The involvement of community structures, traditional and religious leaders, influential individuals, community-based organizations, professional organizations, development partners, relevant government agencies, and hospital management in awareness campaigns, health education, and sensitization on Lassa IPC measures will foster robust and sustainable Lassa fever IPC measures for BDTH and the surrounding community.
4.13. Limitations
The researcher encountered several limitations, including recall bias in self-report questionnaires, non-response from some respondents, and limitations in the generalizability of the study findings. Other limitations were social desirability bias (especially in self-reported IPC practices), access limitations (e.g., staff on leave or unwilling to participate), and getting the attention of very busy clinicians for 30-minute or 1-hour key informant interviews. It is worth noting that measures were taken to address the impact of these limitations on the study’s overall objectives.
4.14. The Need for Further Studies
Healthcare workers, especially clinicians, are critical in practicing Lassa fever IPC in the BDTH, Kaduna. Still, other support staff roles, such as cleaners, security officers, and attendants, should be thoroughly evaluated to inform Lassa Fever IPC policy and regulations in the future. Further studies should also assess the roles of factors, such as funding, policies, leadership, and others, in the effective implementation of Lassa Fever IPC at BDTH, Kaduna.
4.15. Conclusion
Lassa fever remains a significant public health concern in BDTH and the immediate community, and many people have lost their lives to Lassa fever yearly, in addition to the high morbidity. The healthcare worker understood the dynamics of infectious disease, the drivers of Lassa fever infection, and the relationships between host, disease, environment, climate, and biodiversity in initiating and sustaining Lassa fever outbreaks in Kaduna State. They have above-average scores in awareness, knowledge, attitudes, and practices regarding Lassa fever IPC measures, as well as the interrelatedness of global cooperation and partnership with relevant stakeholders in preventing Lassa fever outbreaks. Stopping Lassa Fever outbreaks in Kaduna State requires implementation of critical recommendations to address identified challenges and ensure availability of PPE, water, and sanitation facilities and equipment, rodent control measures, and trained and well-motivated staff on Lassa Fever IPC, who have the optimal knowledge, skills, attitudes, and equipment to detect, control, and prevent Lassa fever outbreaks. Finally, the findings highlight that comprehensive, multi-level interventions targeting both healthcare systems and community engagement are crucial to reducing the burden of Lassa Fever and strengthening public health resilience.
5. Implications for the Intergovernmental Action
The study has shown that Lassa Fever is a zoonotic disease, and interrupting its transmission requires attention to both human and environmental health. The rampant environmental degradation, deforestation, bush burning, and changes in the ecosystem all favor Lassa fever transmission, underscoring the need for effective policies on rodent control and environmental sanitation, as well as a robust synergy between government, health institutions, development partners, and the community.
The study has shown that global cooperation and partnership were critical in response to Lassa fever outbreaks. Nigeria, a signatory to the 2005 International Health Regulations, must report all epidemic-prone diseases to the World Health Organization and take adequate measures to control and prevent outbreaks. It has demonstrated that effective Lassa fever surveillance and response can benefit from financial and technical assistance from international organizations, development partners, and non-government organizations.
6. Conflict of Interest
The author states that there is no conflict of interest.
7. Acknowledgment
I am indeed very grateful to my supervisors, Professors Momodou Mustapha Fanneh and Laurent Cleenewerck for their unwavering guidance, support, and mentorship throughout the entire duration of this thesis. I am equally thankful to my colleagues, Drs. Nauzo Aliyu and Jabani Mamza, for their support and guidance in designing, collecting, and analyzing the research tool. My research assistants, Yakubu Adamu, Tawakaltu Murtala, Fatima Mohammed, Ishaq Abdullahi, Adama Abdullahi, Maryam Yakubu, Hassana Shekarau, Jamilu Sani, Emmanuel Ochai, Patrick Gabriel, Haruna Peter, and Victoria Egah, were wonderful, sacrificial, and supportive throughout. I am very grateful to them for their assistance.
References
Adeke, A.S., R.C. Onoh, C.D. Umeokonkwo, B.N. Azuogu, and E.O. Ogah. ‘Knowledge, Attitude and Practice of Infection Prevention and Control among Healthcare Workers: One Year after an Outbreak of Nosocomial Lassa Fever in a Tertiary Hospital in Southeast NigeriaKnowledge, Attitude and Practice of Infection Prevention and Con’. African Journal of Clinical and Experimental Microbiology 22, no. 4 (2021): 457–64. https://doi.org/10.4314/ajcem.v22i4.5.
Aldhamy, Haifa, Gregory Maniatopoulos, Victoria L. McCune, Ilaf Mansi, Majid Althaqafy, and Mark S. Pearce. ‘Knowledge, Attitude and Practice of Infection Prevention and Control Precautions among Laboratory Staff: A Mixed-Methods Systematic Review’. Antimicrobial Resistance and Infection Control 12, no. 1 (2023). https://doi.org/10.1186/s13756-023-01257-5.
Alhumaid, Saad, Abbas Al Mutair, Zainab Al Alawi, et al. ‘Knowledge of Infection Prevention and Control among Healthcare Workers and Factors Influencing Compliance: A Systematic Review’. Antimicrobial Resistance and Infection Control 10, no. 1 (2021). https://doi.org/10.1186/s13756-021-00957-0.
Alli, Ammar, Juan Fernando Ortiz, Stephanie P Fabara, Amrapali Patel, and Taras Halan. ‘Management of Lassa Fever: A Current Update’. Cureus, ahead of print, Springer Science and Business Media LLC, 2 May 2021. https://doi.org/10.7759/cureus.14797.
Andre, F. E., R. Booy, H. L. Bock, et al. ‘Vaccination Greatly Reduces Disease, Disability, Death and Inequity Worldwide’. Bulletin of the World Health Organization 86, no. 2 (2008): 140–46. https://doi.org/10.2471/BLT.07.040089.
Asgedom, Akeza Awealom. ‘Status of Infection Prevention and Control (IPC) as per the WHO Standardised Infection Prevention and Control Assessment Framework (IPCAF) Tool: Existing Evidence and Its Implication’. Infection Prevention in Practice 6, no. 2 (2024). https://doi.org/10.1016/j.infpip.2024.100351.
Ashinyo, Mary Eyram, Stephen Dajaan Dubik, Vida Duti, et al. ‘Infection Prevention and Control Compliance among Exposed Healthcare Workers in COVID-19 Treatment Centers in Ghana: A Descriptive Cross-Sectional Study’. PLoS ONE 16, no. 3 March (2021). https://doi.org/10.1371/journal.pone.0248282.
Asuke, Sunday, Edgar Agubamah, MuhammedS Ibrahim, and JosephO Ovosi. ‘Knowledge, Attitude, and Practice toward Lassa Fever Prevention and Control among Health Care Providers in Sabon Gari Local Government Area, Kaduna State, Nigeria’. Journal of Medicine in the Tropics 22, no. 1 (2020): 1. https://doi.org/10.4103/jomt.jomt_10_19.
Braun, Virginia, and Victoria Clarke. ‘Conceptual and Design Thinking for Thematic Analysis’. Qualitative Psychology 9, no. 1 (2022): 3–26.
Choi, Ui Yoon, Young Mi Kwon, Hye Jeong Kang, et al. ‘Surveillance of the Infection Prevention and Control Practices of Healthcare Workers by an Infection Control Surveillance-Working Group and a Team of Infection Control Coordinators during the COVID-19 Pandemic’. Journal of Infection and Public Health 14, no. 4 (2021): 454–60. https://doi.org/10.1016/j.jiph.2021.01.012.
Coursera. Coursera: Epidemics – the Dynamics of Infectious Diseases. The Pennsylvania State University.https://www.coursera.org/learn/epidemics/home/module/2.
Dalhat, Mahmood M., Adebola Olayinka, Martin M. Meremikwu, et al. ‘Epidemiological Trends of Lassa Fever in Nigeria, 2018–2021’. PLoS ONE 17, no. 12 December (2022). https://doi.org/10.1371/journal.pone.0279467.
Duvignaud, Alexandre, Marie Jaspard, Ijeoma Chukwudumebi Etafo, et al. ‘Lassa Fever Outcomes and Prognostic Factors in Nigeria (LASCOPE): A Prospective Cohort Study’. The Lancet Global Health 9, no. 4 (2021): e469–78. https://doi.org/10.1016/S2214-109X(20)30518-0.
Eberhardt, Kirsten Alexandra, Johannes Mischlinger, Sabine Jordan, Mirjam Groger, Stephan Günther, and Michael Ramharter. ‘Ribavirin for the Treatment of Lassa Fever: A Systematic Review and Meta-Analysis’. International Journal of Infectious Diseases 87 (October 2019): 15–20. https://doi.org/10.1016/j.ijid.2019.07.015.
Engering, Anneke, Lenny Hogerwerf, and Jan Slingenbergh. ‘Pathogen-Host-Environment Interplay and Disease Emergence’. Emerging Microbes and Infections 2 (2013). https://doi.org/10.1038/emi.2013.5.
Gbadamosi, Faidat Temitope, Tesleem Omotayo Imran, and Hellen Olamijulo. ‘Midwives Knowledge and Attitude on Infection Prevention and Control (IPC)’. Journal of Public Health Sciences 3, no. 03 (2024): 151–58. https://doi.org/10.56741/jphs.v3i03.703.
Harun, Md Golam Dostogir, Md Mahabub Ul Anwar, Shariful Amin Sumon, et al. ‘Pre-COVID-19 Knowledge, Attitude and Practice among Nurses towards Infection Prevention and Control in Bangladesh: A Hospital-Based Cross-Sectional Survey’. PLoS ONE 17, no. 12 December (2022). https://doi.org/10.1371/journal.pone.0278413.
Holt, Andrew, Emilio Hornsey, Anna C. Seale, et al. ‘A Mixed-Methods Analysis of Personal Protective Equipment Used in Lassa Fever Treatment Centres in Nigeria’. Infection Prevention in Practice 3, no. 3 (2021). https://doi.org/10.1016/j.infpip.2021.100168.
Houlihan, Catherine, and Ron Behrens. ‘Lassa Fever’. BMJ (Online) 358 (2017). https://doi.org/10.1136/bmj.j2986.
Ibrahim, Mahmoud A., and Attila Dénes. ‘A Mathematical Model for Lassa Fever Transmission Dynamics in a Seasonal Environment with a View to the 2017–20 Epidemic in Nigeria’. Nonlinear Analysis: Real World Applications 60 (August 2021). https://doi.org/10.1016/j.nonrwa.2021.103310.
Ilesanmi, O S, A O Kareem, A A Afolabi, A J Kareem, and V Ukwenya. ‘Risk Perception, Knowledge, Attitude and Practices Towards Covid-19 and Lassa Fever Prevention among Doctors and Nurses in a Treatment Centre in Nigeria’. In Annals Of Ibadan Postgraduate Medicine, Vol. 19. N.D.
Ireye, Faith, Alphonsus O Aigbiremolen, Olubowale Ekundare Famiyesin, et al. ‘Contact Tracing and Profile of Lassa Fever Contacts in Edo State, Nigeria: Implications for the Control of Lassa Fever Outbreaks’. In J Health Sci Surveillance Sys, vol. 9. no. 1. 2021.
Ireye, Faith, Harrison Ejiyere, Alphonsus O Aigbiremolen, et al. ‘Knowledge, Attitude and Infection Prevention and Control Practices Regarding Lassa Fever among Healthcare Workers in Edo State, Nigeria’. International Journal of Prevention and Treatment 8, no. 1 (2019): 21–27. https://doi.org/10.5923/j.ijpt.20190801.03.
Israel, Glen D. ‘Determining Sample Size’. University of Florida, IFAS Extension PE0D6, no. April 2009 (1992): 1–5. https://doi.org/10.4039/Ent85108-3.
Kamara, Abu Bakarr Steven, Patrick Fatoma, and Andrew Moseray. ‘The Perspectives of Healthcare Professionals on the Strategies, Challenges, and Community Responses to Health System Response and Interventions Towards Lassa Fever Infections and Mortality in Sierra Leone’. Risk Management and Healthcare Policy 17 (2024): 1127–49. https://doi.org/10.2147/RMHP.S455254.
Merson, Laura, Josephine Bourner, Sulaiman Jalloh, et al. ‘Clinical Characterization of Lassa Fever: A Systematic Review of Clinical Reports and Research to Inform Clinical Trial Design’. PLoS Neglected Tropical Diseases 15, no. 9 (2021). https://doi.org/10.1371/journal.pntd.0009788.
Mosadeghrad, Ali Mohammad, Fatemeh Qazanfari, and Sima Keykhani. ‘Hospital Infection Control Accreditation Standards: A Comparative Review’. In Journal of Health and Safety at Work, vol. 12. no. 1. 2022. https://creativecommons.
Naeem, Aroma, Shafaq Zahid, Muhammad Hassan Hafeez, Arifa Bibi, Shehroze Tabassum, and Aymar Akilimali. ‘Re-Emergence of Lassa Fever in Nigeria: A New Challenge for Public Health Authorities’. Health Science Reports 6, no. 10 (2023). https://doi.org/10.1002/hsr2.1628.
National Population Commission. ‘Legal Notice on Publication of 2006 Census Final Results’. Federal Republic of Nigeria Official Gazette 96, no. 2 (2009): B1-42.
Ochu, Chinwe Lucia, Lorretta Ntoimo, Ikenna Onoh, et al. ‘Predictors of Lassa Fever Diagnosis in Suspected Cases Reporting to Health Facilities in Nigeria’. Scientific Reports 13, no. 1 (2023). https://doi.org/10.1038/s41598-023-33187-y.
Okoro, Onyebuchi Augustine, Eniola Bamgboye, Chioma Dan-Nwafor, et al. ‘Descriptive Epidemiology of Lassa Fever in Nigeria, 2012-2017’. Pan African Medical Journal 37, no. 15 (2020): 1–7. https://doi.org/10.11604/pamj.2020.37.15.21160.
Organization, World Health. WHO Report on Global Surveillance of Epidemic-Prone Infectious Diseases. World Health Organization, 2000. http://www.who.int/emc.
Plotkina, Stanley A. ‘Vaccination against the Major Infectious Diseases Vaccination Contre Les Grandespathologies Infectieuses’. Life Sciences 322 (1999).
Qureshi, Mohammed O., Abrar A. Chughtai, and Holly Seale. ‘Recommendations Related to Occupational Infection Prevention and Control Training to Protect Healthcare Workers from Infectious Diseases: A Scoping Review of Infection Prevention and Control Guidelines’. BMC Health Services Research 22, no. 1 (2022). https://doi.org/10.1186/s12913-022-07673-4.
Raabe, Venessa, and Jeffrey Koehler. ‘Laboratory Diagnosis of Lassa Fever’. Journal of Clinical Microbiology 55, no. 6 (2017). https://doi.org/10.1128/JCM.
Riley, Patricia L., Alexandra Zuber, Stephen M. Vindigni, et al. ‘Information Systems on Human Resources for Health: A Global Review’. Human Resources for Health 10, no. 1 (2012): 1. https://doi.org/10.1186/1478-4491-10-7.
Sahiledengle, Biniyam, Azeb Gebresilassie, Tadesse Getahun, and Desta Hiko. ‘Infection Prevention Practices and Associated Factors among Healthcare Workers in Governmental Healthcare Facilities in Addis Ababa’. Ethiopian Journal of Health Sciences 28, no. 2 (2018): 177–86. https://doi.org/10.4314/ejhs.v28i2.9.
Sonpar, Ashlesha, Chandra Omar Hundal, Joan E.E. Totté, et al. ‘Multimodal Strategies for the Implementation of Infection Prevention and Control Interventions—Update of a Systematic Review for the WHO Guidelines on Core Components of Infection Prevention and Control Programmes at the Facility Level’. Clinical Microbiology and Infection 31, no. 6 (2025): 948–57. https://doi.org/10.1016/j.cmi.2025.01.011.
Tahir, Majid Ali, Mumtaz Ali Khan, Aamer Ikram, et al. ‘Assessment of Infection Prevention and Control (IPC) Implementation and Strategies Used for IPC Preparedness at Facility Level in Underdeveloped Areas of Pakistan’. Infection and Drug Resistance 16 (2023): 1997–2006. https://doi.org/10.2147/IDR.S399830.
Tchouaket, Eric Nguemeleu, Idrissa Beogo, Drissa Sia, et al. ‘Protocol for a Systematic Review of Economic Analyses of Nosocomial Infection Prevention and Control Interventions in OECD Hospitals’. BMJ Open 10, no. 7 (2020). https://doi.org/10.1136/bmjopen-2020-037765.
Thazha, Suhas K., Jonas Preposi Cruz, Nahed Alquwez, Bibin Scaria, Sameesh S. Rengan, and Joseph U. Almazan. ‘Infection Prevention and Control Awareness, Attitudes, and Practices among Healthcare Professionals in South India’. Journal of Infection in Developing Countries 16, no. 4 (2022): 659–67. https://doi.org/10.3855/jidc.14746.
Tomczyk, Sara, Anthony Twyman, Marlieke E.A. de Kraker, et al. ‘The First WHO Global Survey on Infection Prevention and Control in Health-Care Facilities’. The Lancet Infectious Diseases 22, no. 6 (2022): 845–56. https://doi.org/10.1016/S1473-3099(21)00809-4.
Ukwenya, Victor Okoliko, Temiloluwa Adeola Fuwape, Tokunbo Ibukun Fadahunsi, and Olayinka Stephen Ilesanmi. ‘Disparities in Knowledge, Attitude, and Practices of Infection Prevention and Control of Lassa Fever among Health Care Workers at the Federal Medical Centre, Owo, Ondo State, Nigeria’. Pan African Medical Journal 38 (2021). https://doi.org/10.11604/pamj.2021.38.357.26208.
Umeh, Gregory C., Laurent Cleenwerck de Kiev, Jabani Mamza, et al. ‘Symptoms of Depression among Outpatients with Suspected COVID-19 in Metropolitan Local Government Areas of Kaduna State, Nigeria’. PLoS ONE 19, no. 5 May (2024). https://doi.org/10.1371/journal.pone.0288567.
Usman, Sulaiman, and Ibrahim Isa Adamu. ‘Modelling the Transmission Dynamics of the Lassa Fever Infection’. Mathematical Theory and Modeling 8, no. 5 (2018). www.iiste.org.
Wudiri, Zara W, Fati L Bukar, John Bimba, Aisha Abdulfathi, Shuaibu J Yahaya, and Babatunji A Omotara. ‘Frontline Insights: An Assessment of Knowledge, Attitude, Infection Prevention, and Control Practices Regarding Lassa Fever among Healthcare Workers in Hospitals in Maiduguri, Borno State’. Kanem Journal of Medical Science, 30 April 2024.
Yun, Nadezhda E., and David H. Walker. ‘Pathogenesis of Lassa Fever’. Viruses 4, no. 10 (2012): 2031–48. https://doi.org/10.3390/v4102031.
[1] Houlihan and Behrens, ‘Lassa Fever’.
[2] Dalhat et al., ‘Epidemiological Trends of Lassa Fever in Nigeria, 2018–2021’.
[3] Yun and Walker, ‘Pathogenesis of Lassa Fever’.
[4] Naeem et al., ‘Re-Emergence of Lassa Fever in Nigeria: A New Challenge for Public Health Authorities’.
[5] Okoro et al., ‘Descriptive Epidemiology of Lassa Fever in Nigeria, 2012-2017’.
[6] Dalhat et al., ‘Epidemiological Trends of Lassa Fever in Nigeria, 2018–2021’.
[7] Organization, WHO Report on Global Surveillance of Epidemic-Prone Infectious Diseases.
[8] Merson et al., ‘Clinical Characterization of Lassa Fever: A Systematic Review of Clinical Reports and Research to Inform Clinical Trial Design’.
[9] Raabe and Koehler, ‘Laboratory Diagnosis of Lassa Fever’.
[10] Ireye et al., ‘Knowledge, Attitude and Infection Prevention and Control Practices Regarding Lassa Fever among Healthcare Workers in Edo State, Nigeria’.
[11] Asuke et al., ‘Knowledge, Attitude, and Practice toward Lassa Fever Prevention and Control among Health Care Providers in Sabon Gari Local Government Area, Kaduna State, Nigeria’.
[12] Adeke et al., ‘Knowledge, Attitude and Practice of Infection Prevention and Control among Healthcare Workers: One Year after an Outbreak of Nosocomial Lassa Fever in a Tertiary Hospital in Southeast Nigeria Knowledge, Attitude and Practice of Infection Prevention and Con’.
[13] Ilesanmi et al., ‘Risk Perception, Knowledge, Attitude and Practices towards Covid-19 and Lassa Fever Prevention among Doctors and Nurses in a Treatment Centre in Nigeria’.
[14] Asuke et al., ‘Knowledge, Attitude, and Practice toward Lassa Fever Prevention and Control among Health Care Providers in Sabon Gari Local Government Area, Kaduna State, Nigeria’.
[15] ilesanmi et al., ‘Risk Perception, Knowledge, Attitude and Practices towards Covid-19 and Lassa Fever Prevention among Doctors and Nurses in a Treatment Centre in Nigeria’.
[16] Kamara et al., ‘The Perspectives of Healthcare Professionals on the Strategies, Challenges, and Community Responses to Health System Response and Interventions Towards Lassa Fever Infections and Mortality in Sierra Leone’.
[17] Wudiri et al., ‘Frontline Insights: An Assessment of Knowledge, Attitude, Infection Prevention, and Control Practices Regarding Lassa Fever among Healthcare Workers in Hospitals in Maiduguri, Borno State’.
[18] Ireye et al., ‘Knowledge, Attitude and Infection Prevention and Control Practices Regarding Lassa Fever among Healthcare Workers in Edo State, Nigeria’.
[19] Duvignaud et al., ‘Lassa Fever Outcomes and Prognostic Factors in Nigeria (LASCOPE): A Prospective Cohort Study’.
[20] Engering et al., ‘Pathogen-Host-Environment Interplay and Disease Emergence’.
[21] Riley et al., ‘Information Systems on Human Resources for Health: A Global Review’.
[22]Coursera., “Coursera: Epidemics – the Dynamics of Infectious Diseases. The Pennsylvania State University.https://www.coursera.org/learn/epidemics/home/module/2’.
[23] Tchouaket et al., ‘Protocol for a Systematic Review of Economic Analyses of Nosocomial Infection Prevention and Control Interventions in OECD Hospitals’.
[24] Plotkina, ‘Vaccination against the Major Infectious Diseases Vaccination Contre Les Grandespathologies Infectieuses’.
[25] Mosadeghrad et al., ‘Hospital Infection Control Accreditation Standards: A Comparative Review’.
[26] Andre et al., ‘Vaccination Greatly Reduces Disease, Disability, Death and Inequity Worldwide’.
[27] Ireye et al., ‘Knowledge, Attitude and Infection Prevention and Control Practices Regarding Lassa Fever among Healthcare Workers in Edo State, Nigeria’.
[28] Ilesanmi et al., ‘Risk Perception, Knowledge, Attitude and Practices towards Covid-19 And Lassa Fever Prevention among Doctors and Nurses in a Treatment Centre in Nigeria’.
[29] Asuke et al., ‘Knowledge, Attitude, and Practice toward Lassa Fever Prevention and Control among Health Care Providers in Sabon Gari Local Government Area, Kaduna State, Nigeria’.
[30] Houlihan and Behrens, ‘Lassa Fever’.
[31] Dalhat et al., ‘Epidemiological Trends of Lassa Fever in Nigeria, 2018–2021’.
[32] Yun and Walker, ‘Pathogenesis of Lassa Fever’.
[33] Dalhat et al., ‘Epidemiological Trends of Lassa Fever in Nigeria, 2018–2021’.
[34] Naeem et al., ‘Re-Emergence of Lassa Fever in Nigeria: A New Challenge for Public Health Authorities’.
[35] Okoro et al., ‘Descriptive Epidemiology of Lassa Fever in Nigeria, 2012-2017’.
[36] Ibrahim and Dénes, ‘A Mathematical Model for Lassa Fever Transmission Dynamics in a Seasonal Environment with a View to the 2017–20 Epidemic in Nigeria’.
[37] Usman and Adamu, ‘Modelling the Transmission Dynamics of the Lassa Fever Infection’.
[38] Ochu et al., ‘Predictors of Lassa Fever Diagnosis in Suspected Cases Reporting to Health Facilities in Nigeria’.
[39] Merson et al., ‘Clinical Characterization of Lassa Fever: A Systematic Review of Clinical Reports and Research to Inform Clinical Trial Design’.
[40] Raabe and Koehler, ‘Laboratory Diagnosis of Lassa Fever’.
[41] Alli et al., ‘Management of Lassa Fever: A Current Update’.
[42] Holt et al., ‘A Mixed-Methods Analysis of Personal Protective Equipment Used in Lassa Fever Treatment Centres in Nigeria’.
[43] Eberhardt et al., ‘Ribavirin for the Treatment of Lassa Fever: A Systematic Review and Meta-Analysis’.
[44] Alli et al., ‘Management of Lassa Fever: A Current Update’.
[45] Ireye et al., ‘Contact Tracing and Profile of Lassa Fever Contacts in Edo State, Nigeria: Implications for the Control of Lassa Fever Outbreaks’.
[46] Sahiledengle et al., ‘Infection Prevention Practices and Associated Factors among Healthcare Workers in Governmental Healthcare Facilities in Addis Ababa’.
[47] Choi et al., ‘Surveillance of the Infection Prevention and Control Practices of Healthcare Workers by an Infection Control Surveillance-Working Group and a Team of Infection Control Coordinators during the COVID-19 Pandemic’.
[48] Ashinyo et al., ‘Infection Prevention and Control Compliance among Exposed Healthcare Workers in COVID-19 Treatment Centers in Ghana: A Descriptive Cross-Sectional Study’.
[49] Alhumaid et al., ‘Knowledge of Infection Prevention and Control among Healthcare Workers and Factors Influencing Compliance: A Systematic Review’.
[50] Qureshi et al., ‘Recommendations Related to Occupational Infection Prevention and Control Training to Protect Healthcare Workers from Infectious Diseases: A Scoping Review of Infection Prevention and Control Guidelines’.
[51] Tomczyk et al., ‘The First WHO Global Survey on Infection Prevention and Control in Health-Care Facilities’.
[52] Thazha et al., ‘Infection Prevention and Control Awareness, Attitudes, and Practices among Healthcare Professionals in South India’.
[53] Gbadamosi et al., ‘Midwives Knowledge and Attitude on Infection Prevention and Control (IPC)’.
[54] Aldhamy et al., ‘Knowledge, Attitude and Practice of Infection Prevention and Control Precautions among Laboratory Staff: A Mixed-Methods Systematic Review’.
[55] Harun et al., ‘Pre-COVID-19 Knowledge, Attitude and Practice among Nurses towards Infection Prevention and Control in Bangladesh: A Hospital-Based Cross-Sectional Survey’.
[56] National Population Commission, ‘Legal Notice on Publication of 2006 Census Final Results’.
[57] Umeh et al., ‘Symptoms of Depression among Outpatients with Suspected COVID-19 in Metropolitan Local Government Areas of Kaduna State, Nigeria’.
[58] Israel, ‘Determining Sample Size’.
[59] Ireye et al., ‘Knowledge, Attitude and Infection Prevention and Control Practices Regarding Lassa Fever among Healthcare Workers in Edo State, Nigeria’.
[60] Ireye et al., ‘Knowledge, Attitude and Infection Prevention and Control Practices Regarding Lassa Fever among Healthcare Workers in Edo State, Nigeria’.
[61] Braun and Clarke, ‘Conceptual and Design Thinking for Thematic Analysis’.
[62] Ukwenya et al., ‘Disparities in Knowledge, Attitude, and Practices of Infection Prevention and Control of Lassa Fever among Health Care Workers at the Federal Medical Centre, Owo, Ondo State, Nigeria’.
[63] Ilesanmi et al., ‘Risk Perception, Knowledge, Attitude and Practices towards Covid-19 and Lassa Fever Prevention among Doctors and Nurses in a Treatment Centre in Nigeria’.
[64] Adeke et al., ‘Knowledge, Attitude and Practice of Infection Prevention and Control among Healthcare Workers: One Year after an Outbreak of Nosocomial Lassa Fever in a Tertiary Hospital in Southeast Nigeria Knowledge, Attitude and Practice of Infection Prevention and Con’.
[65] Kamara et al., ‘The Perspectives of Healthcare Professionals on the Strategies, Challenges, and Community Responses to Health System Response and Interventions Towards Lassa Fever Infections and Mortality in Sierra Leone’.
[66] Asuke et al., ‘Knowledge, Attitude, and Practice toward Lassa Fever Prevention and Control among Health Care Providers in Sabon Gari Local Government Area, Kaduna State, Nigeria’.
[67] Sonpar et al., ‘Multimodal Strategies for the Implementation of Infection Prevention and Control Interventions—Update of a Systematic Review for the WHO Guidelines on Core Components of Infection Prevention and Control Programmes at the Facility Level’.
[68] Asgedom, ‘Status of Infection Prevention and Control (IPC) as per the WHO Standardised Infection Prevention and Control Assessment Framework (IPCAF) Tool: Existing Evidence and Its Implication’.
[69] Tahir et al., ‘Assessment of Infection Prevention and Control (IPC) Implementation and Strategies Used for IPC Preparedness at Facility Level in Underdeveloped Areas of Pakistan’.



